1. Handwashing:
Infectious diseases that are commonly spread through hand-to-hand
contact include the common cold, flu and several gastrointestinal
disorders, such as infectious diarrhea. The combination of the
flu and pneumonia, in fact, is the eighth-leading cause of death
among Americans. Inadequate hand hygiene also contributes to
food-related illnesses, such as salmonella and E. coli infection.
According to the Centers for Disease Control and Prevention
(CDC), as many as 76 million Americans get a food-borne illness
each year. Of these, about 5,000 die as a result of their illness.
Others experience the annoying signs and symptoms of nausea,
vomiting and diarrhea. Good hand-washing techniques include
washing your hands with soap and water or using an alcohol-based
hand sanitizer. Antimicrobial wipes or towelettes are just as
effective as soap and water in cleaning your hands but aren't
as good as alcohol-based sanitizers. Antibacterial soaps have
become increasingly popular in recent years. However, these
soaps are no more effective at killing germs than is regular
soap. Using antibacterial soaps may lead to the development
of bacteria that are resistant to the products' antimicrobial
agents — making it even harder to kill these germs in
the future. In general, regular soap is fine. The combination
of scrubbing your hands with soap — antibacterial or not
— and rinsing them with water loosens and removes bacteria
from your hands.( http://www.mayoclinic.com/health/hand-washing/HQ00407)
# Wet your hands with warm, running water and
apply liquid soap or use clean bar soap. Lather well.
# Rub your hands vigorously together for at least 15 to 20 seconds.
# Scrub all surfaces, including the backs of your hands, wrists,
between your fingers and under your fingernails.
# Rinse well.
# Dry your hands with a clean or disposable towel.
2. Isolation Procedures:
Standard Precautions-
Assume that every person is potentially infected or colonized
with an organism that could be transmitted in the healthcare
setting and apply the following infection control practices
during the delivery of health care. Combines the major features
of Universal Precautions (UP) and Body Substance Isolation (BSI)
and are based on the principle that all blood, body fluids,
secretions, excretions except sweat, nonintact skin, and mucous
membranes may contain transmissible infectious agents. Standard
Precautions include a group of infection prevention practices
that apply to all patients, regardless of suspected or confirmed
infection status, in any setting in which healthcare is delivered.
These include: hand hygiene; use of gloves, gown, mask, eye
protection, or face shield, depending on the anticipated exposure;
and safe injection practices. Also, equipment or items in the
patient environment likely to have been contaminated with infectious
body fluids must be handled in a manner to prevent transmission
of infectious agents (e.g., wear gloves for direct contact,
contain heavily soiled equipment, properly clean and disinfect
or sterilize reusable equipment before use on another patient).
New elecments of standard precaution include: Respiratory Hygiene/Cough
Etiquette, safe injection practices, and use of masks for insertion
of catheters or injection of material into spinal or epidural
spaces via lumbar puncture procedures (e.g., myelogram, spinal
or epidural anesthesia). While most elements of Standard Precautions
evolved from Universal Precautions that were developed for protection
of healthcare personnel, these new elements of Standard Precautions
focus on protection of patients.
- The transmission of SARS-CoV in emergency departments by patients
and their family members during the widespread SARS outbreaks
in 2003 highlighted the need for vigilance and prompt implementation
of infection control measures at the first point of encounter
within a healthcare setting (e.g., reception and triage areas
in emergency departments, outpatient clinics, and physician
offices).
- Healthcare personnel are advised to observe
Droplet Precautions (i.e., wear a mask) and hand hygiene when
examining and caring for patients with signs and symptoms of
a respiratory infection. Healthcare personnel who have a respiratory
infection are advised to avoid direct patient contact, especially
with high risk patients. If this is not possible, then a mask
should be worn while providing patient care.
Transmission Based Precautions-
There are three categories of Transmission-Based Precautions:
Contact Precautions
Droplet Precautions
Airborne Precautions.
Transmission-Based Precautions are used when the route(s) of
transmission is (are) not completely interrupted using Standard
Precautions alone. For some diseases that have multiple routes
of transmission (e.g., SARS), more than one Transmission-Based
Precautions category may be used. When used either singly or
in combination, they are always used in addition to Standard
Precautions.
Contact Precautions-
Contact Precautions are intended to prevent transmission of
infectious agents, including epidemiologically important microorganisms,
which are spread by direct or indirect contact with the patient
or the patient's environment. ontact Precautions also apply
where the presence of excessive wound drainage, fecal incontinence,
or other discharges from the body suggest an increased potential
for extensive environmental contamination and risk of transmission.
A single patient room is preferred for patients who require
Contact Precautions. Healthcare personnel caring for patients
on Contact Precautions should wear a gown and gloves for all
interactions that may involve contact with the patient or potentially
contaminated areas in the patient's environment. Donning PPE
before room entry and discarding before exiting the patient
room is done to contain pathogens, especially those that have
been implicated in transmission through environmental contamination
Droplet Precautions-
Droplet Precautions are intended to prevent transmission of
pathogens spread through close respiratory or mucous membrane
contact with respiratory secretions.. Because these pathogens
do not remain infectious over long distances in a healthcare
facility, special air handling and ventilation are not required
to prevent droplet transmission. Droplet Precautions are indicated
are for conditions such as. pertussis, influenza virus, adenovirus,
rhinovirus, N. meningitides, and group A streptococcus.Healthcare
personnel wear a mask (a respirator is not necessary) for close
contact with infectious patient; the mask is generally donned
upon room entry. Patients on Droplet Precautions who must be
transported outside of the room should wear a mask if tolerated
and follow Respiratory Hygiene/Cough Etiquette. Use Droplet
Precautions for patients known or suspected to be infected with
pathogens transmitted by respiratory droplets (i.e., large-particle
droplets >5µ in size) that are generated by a patient
who is coughing, sneezing or talking.
Airborne Precautions-
Airborne Precautions prevent transmission of infectious agents
that remain infectious over long distances when suspended in
the air (e.g., rubeola virus [measles], varicella virus [chickenpox],
Mycobacterium. tuberculosis, and possibly SARS-CoV). The preferred
placement for patients who require Airborne Precautions is in
an airborne infection isolation room (AIIR). An AIIR is a single-patient
room that is equipped with special air handling and ventilation
capacity that meet the American Institute of Architects/Facility
Guidelines Institute (AIA/FGI) standards for AIIRs (i.e., monitored
negative pressure relative to the surrounding area, 12 air exchanges
per hour for new construction and renovation and 6 air exchanges
per hour for existing facilities, air exhausted directly to
the outside or recirculated through HEPA filtration before return).In
settings where Airborne Precautions cannot be implemented due
to limited engineering resources (e.g., physician offices),
masking the patient, placing the patient in a private room (e.g.,
office examination room) with the door closed, and providing
N95 or higher level respirators or masks if respirators are
not available for healthcare personnel will reduce the likelihood
of airborne transmission until the patient is either transferred
to a facility with an AIIR or returned to the home environment,
as deemed medically appropriate. Whenever possible, non-immune
HCWs should not care for patients with vaccine-preventable airborne
diseases (e.g., measles, chickenpox, and smallpox).(http://www.cdc.gov/ncidod/dhqp/gl_isolation_droplet.html)
3. Ventilator Associated Pneumonia- (VAP Considerations)
Ventilator Associated Pneumonia is a nosocmial pneumonia that
develops in a patient intubated for 48 hours or more. Pneumonia
has accounted for approximately 15% of all hospital-associated
infections and 27% and 24% of all infections acquired in the
medical intensive-care unit (ICU) and coronary care unit, respectively.
It has been the second most common hospital-associated infection
after that of the urinary tract. The primary risk factor for
the development of hospital-associated bacterial pneumonia is
mechanical ventilation (with its requisite endotracheal intubation).
Oral hygiene has been proven to help reduce healthcare-acquired
pneumonias (HAPs), including ventilator-associated pneumonia
(VAP) and aspiration pneumonia. In fact, the CDC now requires
acute care hospitals to “develop and implement a comprehensive
oral hygiene program" for patients at risk for healthcare-associated
pneumonia. The CDC’s National Nosocomial Infection Surveillance
System (NNIS) reported that in 2002, the median rate of VAP
per thousand ventilator-days in NNIS hospitals ranged from 2.2
in pediatric ICUs to 14.7 in trauma ICUs. In other reports,
patients receiving continuous mechanical ventilation had 6-21
times the risk of developing hospital-associated pneumonia compared
with patients who were not receiving mechanical ventilation.
Because of this tremendous risk, in the last two decades, most
of the research on hospital-associated pneumonia has been focused
on VAP. (http://www.cdc.gov/ncidod/dhqp/dpac_ventilate_data.html)
Reference Document: VAP
Reference Document
4. Drug Resistant Organisims-
Antibiotic resistance has been called one of the world's most
pressing public health problems. Almost every type of bacteria
has become stronger and less responsive to antibiotic treatment
when it is really needed. These antibiotic-resistant bacteria
can quickly spread to family members, schoolmates, and co-workers
- threatening the community with a new strain of infectious
disease that is more difficult to cure and more expensive to
treat. For this reason, antibiotic resistance is among CDC's
top concerns. Antibiotic resistance can cause significant danger
and suffering for children and adults who have common infections,
once easily treatable with antibiotics. Microbes can develop
resistance to specific medicines. A common misconception is
that a person's body becomes resistant to specific drugs. However,
it is microbes, not people, that become resistant to the drugs.
If a microbe is resistant to many drugs, treating the infections
it causes can become difficult or even impossible. Someone with
an infection that is resistant to a certain medicine can pass
that resistant infection to another person. In this way, a hard-to-treat
illness can be spread from person to person. In some cases,
the illness can lead to serious disability or even death.
Antibiotic resistance occurs when bacteria change in some way
that reduces or eliminates the effectiveness of drugs, chemicals,
or other agents designed to cure or prevent infections. The
bacteria survive and continue to multiply causing more harm.
Bacteria can do this through several mechanisms. Some bacteria
develop the ability to neutralize the antibiotic before it can
do harm, others can rapidly pump the antibiotic out, and still
others can change the antibiotic attack site so it cannot affect
the function of the bacteria.
Antibiotics kill or inhibit the growth of susceptible bacteria.
Sometimes one of the bacteria survives because it has the ability
to neutralize or escape the effect of the antibiotic; that one
bacterium can then multiply and replace all the bacteria that
were killed off. Exposure to antibiotics therefore provides
selective pressure, which makes the surviving bacteria more
likely to be resistant. In addition, bacteria that were at one
time susceptible to an antibiotic can acquire resistance through
mutation of their genetic material or by acquiring pieces of
DNA that code for the resistance properties from other bacteria.
The DNA that codes for resistance can be grouped in a single
easily transferable package. This means that bacteria can become
resistant to many antimicrobial agents because of the transfer
of one piece of DNA. Listen
to Drug Resistant Antibiotics - PODCAST
What is multidrug-resistant tuberculosis (MDR TB)?
* Multidrug-resistant tuberculosis (MDR TB) is TB that is
resistant to at least two of the best anti-TB medications, isoniazid
and rifampin. These medications are considered first-line drugs
and are used to treat all persons with drug-susceptible TB disease.
* A more serious form of MDR TB is called extensively drug-resistant
TB (XDR TB). XDR TB is a relatively rare type of TB that is
resistant to nearly all medicines used to treat TB disease.
Because XDR TB is resistant to the most effective TB medicines
used to treat TB, patients are left with very limited useful
treatment options.
* Treatment for MDR TB is considerably less effective, more
toxic, and more expensive than for drug-susceptible TB. MDR
TB, as is XDR TB, is a difficult to treat disease that is often
fatal.
* Treatment of MDR TB requires a patient to take 18–24
months of medication, including taking multiple second-line
medications, to kill the bacteria.
MRSA-
Methicillin-resistant Staphylococcus aureus (MRSA) is a type
of bacteria that is resistant to certain antibiotics. These
antibiotics include methicillin and other more common antibiotics
such as oxacillin, penicillin and amoxicillin. Staph infections,
including MRSA, occur most frequently among persons in hospitals
and healthcare facilities (such as nursing homes and dialysis
centers) who have weakened immune systems. MRSA infections that
occur in otherwise healthy people who have not been recently
(within the past year) hospitalized or had a medical procedure
(such as dialysis, surgery, catheters) are known as community-associated
(CA)-MRSA infections. These infections are usually skin infections,
such as abscesses, boils, and other pus-filled lesions. The
main mode of transmission to other patients is through human
hands, especially healthcare workers' hands. Hands may become
contaminated with MRSA bacteria by contact with infected or
colonized patients. If appropriate hand hygiene such as washing
with soap and water or using an alcohol-based hand sanitizer
is not performed, the bacteria can be spread when the healthcare
worker touches other patients. MRSA is becoming more prevalent
in healthcare settings. According to CDC data, the proportion
of infections that are antimicrobial resistant has been growing.
In 1974, MRSA infections accounted for two percent of the total
number of staph infections; in 1995 it was 22%; in 2004 it was
63%..(http://www.cdc.gov/ncidod/dhqp/ar_MRSA_spotlight_2006.html). Listen
to Methicillin-Resistant Staphylococcus Aureus (MRSA)- PODCAST
5. Sterilization/Disenfection Disenfection- Disinfection is using an agent
that destroys germs or other harmful microbes or inactivates
them, usually referred to chemicals that kill the growing forms
(vegetative forms) but not the resistant spores of bacteria. Sterilization- Any process, physical or chemical,
that will destroy all forms of life, including bacterial, mold,
spores, and viruses. Antisepsis- Destruction of pathogenic microorganisms
existing in their vegetative state on living tissue Sanitize- To reduce the population of microbes
on inanimate objects to a safe level as judged by public health
authorities
Autoclaving-
Sterilizization of any equipment that is properly prepared and
processed. Combines high heat, moisture, and pressure: Temp.=121-126°C
@1-2Atm.Equipment must be washed with a detergent, rinsed, and
then packaged in a porous material, e.g., milar Typical settings
are 121°C @ 15 psi for 15 min. or 121°C @ 30 psi for
3 min. Indicator tape changes color to verify if exposure sufficient
for sterilization. Melts most plastics, can dull surgical instruments.
Cannot be used on electronic devices.
Pasteurization-
Involves heating a liquid to temperatures sufficient to destroy
vegetative organsims. Equipment is immersed in hot water bath
at 63°C for 30 min. Disinfects, does not sterilize. The
moist heat coagulates the cellular protein of microbes. Spores
are not destroyed. Prepare equipment by disassembling, washing
in detergent, and then rinsing. After pasteurization remove
equipment and place in drying cabinet. When dry, assemble, package
and date equipment. Advantages of pasteurization include: safe
for plastics, less expensive than chemicals, no employee exposure
to chemicals.
Ethylene Oxide-
Is a toxic gas that is combined with moisture and heat to sterilize
equipment. Effectiveness depends on equipment prep., gas [ ],
humidity, and temp. Works by affecting the enzymes, reproduction,
and metabolism of microbes.
Prepare equipment by washing in detergent, rinsing, and allow
to dry (ethylene glycol). After drying, place in porous package.
Expose package to gas [ ] of 800-1000 mg/L that is mixed with
CO2 or freon (decreased explosion hazard), 49-57°C, 30-60%
humidity, for 3-4 hours. After EtO, aerate equip. in special
cabinet for 12 hr. - several days, depending on material.
Glutaraldehyde-
Chemical used to cold sterilize or disinfect equipment by immersion.
“Cidex” is most common example. Can be alkaline
or acid glutaraldehyde. Disassemble equipment, wash in detergent,
rinse, shake dry, and immerse in glutaraldehyde. Alkaline glutaraldehyde.
- disinfection after 10 min., sterilization after 10 hours.
Acid glutaraldehyde. - disinfection. after 20 min.. After immersion,
rinse with sterile water or bleach solution and allow to dry
in a drying cabinet. Dermal sensitivity or allergy to fumes
with some people. Good for rubber and plastic, not electronic
equipment. Life of product varies from 14 - 30 days.
Alcohols-
Ethyl and isopropyl are most common disinfectants. 70% isopropyl
is bactericidal and fungicidal but not sporacidal. Work by damaging
cell walls.
B. PATIENT ASSESSMENT
1. Breath Sounds
Breath sounds can be classified into two categories, either
NORMAL or ABNORMAL (adventitious). Breath sounds originate in
the large airways where air velocity and turbulence induce vibrations
in the airway walls. These vibrations are then transmitted through
the lung tissue and thoracic wall to the surface where they
may be heard readily with the aid of a stethescope. Normal breath
sound production is directly related to air flow velocity and
airway lumen architecture. Air flow velocity is primarily determined
by pulmonary ventilation (minute volume ® velocity)
and TOTAL cross sectional airway area ( area ® velocity)
at any given level in the lungs.
Normal Breath Sounds-
Bronchial Sounds
Bronchial breath sounds consist of a full inspiratory and expiratory
phase with the inspiratory phase usually being louder. They
are normally heard over the trachea and larynx. Bronchial sounds
are not normally heard over the thorax.. They may be heard over
the hilar region in normal animals that are breathing hard (i.e.
after exercise). Otherwise, bronchial sounds heard over the
thorax suggest lung consolidation and pulmonary disease. Pulmonary
consolidation results in improved transmission of breath sounds
originating in the trachea and primary bronchi that are then
heard at increased intensity over the thorax. Listen
to- Bronchail Breath Sounds
Bronchovesicular Sounds
Bronchovesicular breath sounds consist of a full inspiratory
phase with a shortened and softer expiratory phase. They are
normally heard over the hilar region in most resting individuals
and should be quieter than the tracheal breath sounds. Increased
intensity of bronchovesicular sounds is most often associated
with increased ventilation or pulmonary consolidation. Listen
to_ Bronchovesicular Breath Sounds
Vesicular Sounds
Vesicular breath sounds consist of a quiet, wispy inspiratory
phase followed by a short, almost silent expiratory phase. They
are heard over the periphery of the lung field. As stated earlier,
these sounds are NOT produced by air moving through the terminal
bronchioles and alveoli but rather are the result of attenuation
of breath sounds produced in the bronchi at the hilar region
of the lungs. These sounds may be absent or silent in the periphery
of normal resting animals. They are highly variable in intensity
depending on the species, ventilation, and body condition. Increased
intensity may be associated with pulmonary consolidation. Listen
to- Vesicular Breath Sounds
Abnormal Breath Sounds
Crackles
Crackles are discontinuous, explosive, "popping" sounds
that originate within the airways. They are heard when an obstructed
airway suddenly opens and the pressures on either side of the
obstruction suddenly equilibrates resulting in transient, distinct
vibrations in the airway wall. The dynamic airway obstruction
can be caused by either accumulation of secretions within the
airway lumen or by airway collapse caused by pressure from inflammation
or edema in surrounding pulmonary tissue. Crackles can be heard
during inspiration when intrathoracic negative pressure results
in opening of the airways or on expiration when thoracic positive
pressure forces collapsed or blocked airways open. Crackles
are heard more commonly during inspiration than expiration.
They are significant as they imply either accumulation of fluid
secretions or exudate within airways or inflammation and edema
in the pulmonary tissue. Listen
to- Crackles
Wheezes
Wheezes are continuous musical tones that are most commonly
heard at end inspiration or early expiration. They result as
a collapsed airway lumen gradually opens during inspiration
or gradually closes during expiration. As the airway lumen becomes
smaller, the air flow velocity increases resulting in harmonic
vibration of the airway wall and thus the musical tonal quality.
Wheezes can be classified as either high pitched or low pitched
wheezes. It is often inferred that high pitch wheezes are associated
with disease of the small airways and low pitch wheezes are
associated with disease of larger airways. However, this association
has not been confirmed. Wheezes may be monophonic (a single
pitch and tonal quality heard over an isolated area) or polyphonic
(multiple pitches and tones heard over a variable area of the
lung). Wheezes are significant as they imply decreased airway
lumen diameter either due to thickening of reactive airway walls
or collapse of airways due to pressure from surrounding pulmonary
disease. Listen
to- Wheezes
Stridor
Stridor are intense continuous monophonic wheezes heard loudest
over extrathoracic airways. They tend to be accentuated during
inspiration when extrathoracic airways collapse due to lower
internal lumen pressure. They can often be heard without the
aid of a stethoscope. Careful auscultation with a stethoscope
can usually identify an area of maximum intensity that is associated
with the airway obstruction. This is typically either at the
larynx or at the thoracic inlet. These extrathoracic sounds
are often referred down the airways and can often be heard over
the thorax and are often mistaken as pulmonary wheezes. Stridor
is significant and indicates upper airway obstruction. Listen
to- Stridor
Vocal Sounds
Egophony
Egophony is the Greek word for "Voice of the Goat".
This sound is the "EEEEE" to "AAAAA" conversion
that a person will make when being asked to say "EEEEE"
while the auscultator listens to the lungs which is heard by
the auscultator as "AAAAA" through the stethoscope. Listen
to- Egophony
Whispered Pectoriloquy
Whispered Pectoriloquy is the sound that is heard through the
stethoscope by the auscultator when the patient whispers a word
or a number. Normally, whispered sounds are not heard through
the chest wall. Because of fluid buildup in the alveolar regions
of the lung, the whispered sound can be heard distinctly. Listen
to- Whispered Pectoriloquy
Chest Assessment
Palpation
The chest and lung transmit a vibration, called fremitus, during
speech. Fremitus abnormalities may be felt in chronic obstructive
lung diseases or obesity, in which the vibration is diminished,
and in pneumonia, in which it is increased over the infected
lobe. Determine the range of respiratory movement (how far the
chest expands when he inhales and how far the chest contracts
when he exhales). You can also feel symmetry of respiratory
movement (whether or not the body parts feel the same on both
sides during a respiration).
Percussion:
Tapping on the chest wall over healthy lung results in a hollow
resonant sound. The hollow character of the resonance sometimes
is exaggerated in emphysematous lungs or in pneumothorax, and
muffled by pleural effusions or pulmonary consolidation.
Tactile Fremitus
When a person speaks, vibrations that can be felt are transmitted
through the bronchopulmonary system to the chest wall. These
vibrations can best be felt when a person says the words "ninety-nine"
or "one-oneone." Ask the person to speak louder or
lower his head if you cannot feel the vibrations.
Vital Signs
Blood Pressure Blood pressure is the
pressure exerted on the wall of the artery or vein as blood
is pumped through the body. Blood does not flow readily, it
surges along with each beat of the heart. The walls of the arteries
are thicker than the veins and as such much more force is generated
allowing us to record that pressure.As the blood
is pumped through the vessels a turbulence is heard. These sounds
are created by turbulence as the blood begins to flow through
the arteries after the blood pressure cuff has temporarily stopped
the flow by the pressure exerted as it was inflated. When the
sound is first heard, this is the systolic pressure; and when
the sound ceases as the turbulence ends, the diastolic pressure
is determined. As blood is pumped through the body it exerts
pressure on the veins and arteries. The systolic pressure is
the pressure as the heart contracts and pumps the blood. The
diastolic pressure is the pressure in the vessels when the heart
is at rest between beats. Blood pressure is recorded as a fraction
such as 110/70. The systolic pressure is the top number and
the diastolic number is the bottom number. Read more: http://healthfieldmedicare.suite101.com/article.cfm/vital_signs__blood_pressure#ixzz0TBMPojUd Video
of How to take a Blood pressure
Pulse
The pulse is checked as one indicator of abnormalities of the
heart by observing the rate, rhythm, and the strength and tension
of the beat against the arterial wall. The pulse may be recorded
hourly to every four hours, or p.r.n. (when required), based
on the patient's condition. For example, the pulse may be recorded
postoperatively every 15 minutes in the recovery room. The average
heart rate for older children and adults can range from 50 to
90 beats per minute (bpm). This is an average; rates vary between
males and females, with age, and with the patient's health and
level of fitness. It is not abnormal for athletes to display
a low pulse rate.
The pulse is an indicator of the health of the heart and the
arterial circulation. Such factors as anxiety, medication, or
pulmonary disease may also cause the heart rate to be faster
or slower. A low-volume, or weak, pulse may be caused by a number
of factors, including myocardial infarction, shock, intracranial
pressure, or the use of vasoconstrictor drugs. Pulse pressure
may become raised due to arteriosclerosis, as the heart has
to pump harder to promote the flow of blood around the body.
This high-pressure pulse is called a bounding pulse, and may
also be caused by such conditions as fever, pregnancy, or thyrotoxicosis.
It may also be an indicator that pulmonary disease is present.
Respiratory Rate
The number of breaths per minute or, more formally, the number
of movements indicative of inspiration and expiration per unit
time. In practice, the respiratory rate is usually determined
by counting the number of times the chest rises or falls per
minute. By whatever means, the aim is to determine if the respirations
are normal, abnormally fast (tachypnea), abnormally slow (bradypnea),
or nonexistent (apnea). Normal respiratyr rate is about 10-20
breaths per minute. Hypoxemia can result in an increased respiratory
rate and certain drugs or injuries to the brain stem can cause
a fall in baseline respiratory rate.
Temperature
Normal" body temperature as an oral temperature is around
98.6 °F. This is an average of normal body temperatures.
Your temperature may actually be 1°F or more above or below
98.6 °F. Also, your normal body temperature changes by as
much as 1°F throughout the day, depending on how active
you are and the time of day. Temperature readings, even in the
same individual, may be different in different regions of the
body, and may be influenced by the ambient temperature and other
external factors. Body temperature is very sensitive to hormone
levels and may be higher or lower when a woman is ovulating
or having her menstrual period.
In most adults, an oral temperature above 100 °F (37.8 °C)
or a rectal or ear temperature above 101 °F (38.3 °C)
is considered a fever. A child has a fever when his or her rectal
temperature is 100.4 °F (38 °C) or higher.
Infections is the most common cause of a fever. Infections may
affect the whole body or a specific body part (localized infection).
• Medications, such as antibiotics, narcotics, barbiturates,
antihistamines, and many others. These are called drug fevers.
Some medications, such as antibiotics, raise the body temperature
directly; others interfere with the body's ability to readjust
its temperature when other factors cause the temperature to
rise.
• Severe trauma or injury, such as a heart attack, stroke,
heat exhaustion or heatstroke, or burns.
• Other medical conditions, such as arthritis, hyperthyroidism
and even some cancers, such as leukemia, Hodgkin’s lymphoma,
and liver and lung cancer. Can a low body temperature be dangerous
An abnormally low body temperature (hypothermia) can be serious,
even life-threatening. Low body temperature may occur from cold
exposure, shock, alcohol or drug use, or certain metabolic disorders,
such as diabetes or hypothyroidism. A low body temperature may
also be present with an infection, particularly in newborns,
older adults, or people who are frail. An overwhelming infection
may also cause an abnormally low body temperature. Medical Records/Charting
The patient medical record serves as the official medical documentation.
It can be either in paper format or digital (paperless). The
record contains confidential information and is protected under
the HIPPA regulations. Patient information should not be shared
or accessed by anyone not having a direct care relationship
with that patient. Respiratory Therapsist's document in the
medical record sush things as therapies administered, alterations
in the plan of care (TDP's) and patient condition changes (progress
notes).
Respiratory Care Notes:
SOAP- A form of patient notation that documents
in the following four domain areas:
Subjective- Findings in the words of the patient such as "
I am having chest pain"
Objective- Patient assessment and other pertinent data.
Assessment- Problem list of patient (potential diagnosis and
findings)
Plan- Modifications and or reccomendations to the plan of care
Therapist Driven Protocols (TDP's)
Respiratory care protocols, also called therapist-driven protocols
and patient-driven protocols, are structured guide-lines for
respiratory therapies that are implemented, adjusted, and discontinued
by respiratory care practitioners (RCPs) under physician oversight.
The main impetus for respiratory protocols is to enhance appropriate
prescription of respiratory care services and/or to minimize
misallocation, which has been shown to occur commonly in many
types of health care institutions and for a broad range of respiratory
care services.
Available studies reporting misallocation of respiratory care,
consists both of "overordering" and of "under-ordering"
respiratory care. Most studies focus on "over-ordering"
(ie, ordering services that are unlikely to provide clinical
benefit), the frequency of which ranges from 25% (for 5 respiratory
care services examined by Kester and Stoller7) to 61% for bronchopulmonary
hygiene.9-10 Studies published since the earlier review show
similar rates of misallocation. For example, in an examination
of bronchopulmonary hygiene ordering at University of California
Los Angeles (UCLA) Medical Center, Alexander et al10 reported
that orders for 59.6% of patients examined were deemed inappropriate.
In summary, available evidence suggests the following conclusions:
1. Misallocation of respiratory care services is common, and
occurs in many types of health care institutions (eg, adult
and pediatric, academic and private) and for a variety of respiratory
care services.
2. Both over-ordering and under-ordering occur. Although over-ordering
seems more common, the paucity of available studies and the
sampling frames considered suggest that reported frequencies
of under-ordering are underestimates.
Possible Reasons for Misallocation of Respiratory Care Services
Understanding the reasons that misallocation occurs can suggest
strategies to lessen misallocation. Though sparsely studied,
three possible reasons have been proposed:
1. Respiratory care conditions are frequently misdiagnosed,
leading to the prescription of inappropriate therapies.
2. Respiratory care treatments are prescribed more cavalierly
than drugs, with inadequate attention to appropriate dose and
frequency.
3. Health care providers who are empowered to order respiratory
care services lack appropriate knowledge about rlying principles
to make optimal prescribing decisions.
Oxygen
21% O2 in atmosphere, partial pressure varies with barometric
pressure. Normal at 1 atmophere (760 mmHg) is PO2 of 159 mmHg.
Supports combustion, nonflammable
Be careful around petroleum products- influence ignition of
oxygen.
Oxygen has paramagnetic properties
Fractional Distillation is the method for manufacturing oxygen
commercially.
Medical Gas Distribution Systems
Liquid Reservoir Systems (Bulk Supply)
Stored liquid oxygen at a temp of -183 Celsius
1: 861 ratio. 1 cubic foot of liquid oxygen expands to 861 feet
of gaseous oxygen.
This is allows for large amounts of storage.
Liquid is vaporized to a gas and
reduced to a pressure of 50 psi and
fed into hospital piping systems.
Oxygen Cylinders
Oxygen cylinders (compressed gas)
Available in variety of sizes. Employs Safety Connections (PISS
& DISS)
H & E cylinders most common in hospital.
H cylinder weighs 135 lbs contains 244 cu/ft O2
E cylinder weighs 16 lbs contains 22 cu/ft O2
Cylinder construction regulated by DOT
Cylinder labeling regulated by FDA
Oxygen Regulators & Flowmeters
Regulators or reducing valves reduce pressure to a working pressure.
Many different types of reducing valves: single stage, double
stage etc..
Flowmeters are used to control and indicate flow.
Flowmeters operate by restriction of flow with a variable orifice.
Bourdon Guage and Thorpe Tube are common types of flowmeters.
Bourdon Gauge
Used in oxygen transport.
Backpressure downstream will result in inaccurate flow readings
(higher flow reading then actual delivererd.)
Flow is accurately displayed regardless of tank position.
Should not be used with nebulizers and other devices that increase
downstream pressures.
Thorpe Tube Flowmeters
Operate using a variable orifice.
Employs needle valve and float.
Needle valve controls flow.
Float (little ball) measures flow.
Can be pressure compensated or non-pressure compensated devices.
Pressure compensated most commonly used and reads “accurate”
in the face of back pressure.
Oxygen Therapy Delivery Devices
Divided into High Flow or Low Flow devices.
Low flow device may not meet patient inspiratory flow demands..
Delivered FIO2 not guaranteed.
High Flow devices typically provide enough total flow to meet
inspiratory demands therefore delivering a more accurate FIO2.
High flow does not necessarily mean High FIO2!
Nasal Cannula
Low Flow Device. Typically used between 1-6 lpm
Most commonly used O2 device. Delivered FIO2 dependent on two
factors:
Set Flow and patients inspiratory flow. Humidify flow at 4 liters
or above.
Estimated delivered FIO2 for flow rates:
1 liters= 24% 2 liters= 28%
3 liters= 32% 4 liters= 36%
5 liters= 40% 6 liters= 44%
Simple Oxygen Mask
Oxygen flow rate setting 5-12 lpm
Low flow device
FiO2 delivery range 30%-60% depending on set flow rate and depth
of breathing (tidal volume/minute volume.)
Minimum flow of 5L needs to be set to prevent CO2 re-breathing.
Should only be used for short periods of time in the event a
Cannula is not available.
May or may not be humidified.
Partial Re-Breathing Mask
Basically a simple mask with reservoir bag attached. Low flow
device.
Set flow between 8-15 Lpm to assure reservoir bag is at least
half full during inspiration.
The first 1/3 of expired gas enters the reservoir bag. No one
way valves between bag and mask.
Delivered FIO2 range between 40%- 70%.
Non-Rebreathing Mask
Considered high or Low flow device. Incorporation of 1 way valves
on mask and above reservoir bag.
One way valve over reservoir bag prevents expired gas from entering
bag.
One way valve(s) over the ports limits entrainment of room air.
Typical minimum set flow rates 10-15 Lpm.
Bag should not collapse on inspiration.
Delivered FIO2 60-80% with 1 valve. Up to 100% with two port
valves attached.
Air Entrainment Masks
Venturi Mask. High flow device.
FIO2 range 24%-50%. Set flow rate dependent on selected FIO2
adapter
Components: mask, jet, entrainment ports.
Principle of operation: Viscous shearing forces of gas through
jet entrains room air.
Delivered FIO2 dependent on jet size, flow rate and entrainment
port size.
Lower FIO2’s= higher total flows and vice/versa. Entrainment Ratios Chart
Fi02 Setting Oxygen Flow Entrainment Ratio Total Flow
24% 4 liters 1:25 104 LPM
28% 4 liters 1:10 44 LPM
31% 6 liters 1:7 48 LPM
35% 8 liters 1:5 48 LPM
40% 8 liters 1:3 32 LPM
50% 12 liters 1:1.7 32 LPM
60% 12 liters 1:1 24 LPM
70% 12 liters 1:0.6 19 LPM Calculate Total Flow Oxygen liter flow multiplied by the air entrainment
ratio:
35% venturi mask running at 8 liters, what is the total flow?
1:5 ratio for a 35% mask (6 x 8= 48 liters)
In the case of a 1:5 ratio, the “1” represents the
oxygen flow and the “5” represents the airflow.
In other words, you have (1 x 8= 8 liters O2)
You have 5 x 8= 40 liters of O2
Total flow= 48 liters
Jet Nebulizer High Flow System
Works on Bernoulli’s principle
FiO2 range 28%-100%
Flowmeter should be set between 8 liters & flush
Can be used with aerosol mask, t-piece, trach collar or face
tent.
Water condensation in tubing will create back pressure resulting
in a increase in delivered FIO2 but a decrease in total flow
delivery.
Can be heated to help with secretion maintenance
Jet Nebulizer Components
Gas Injection Nebulizer (GIN) High Flow device. Deliver 100% FIO2 at 40 liters
Can be hooked to the 50 psi high pressure outlet.
Cab be run off air or oxygen gas source depending on desired/range
of FIO2.
Accessory tube acts as a bleed in. FIO2 should be analyzed.
Oxygen Calculations & Equations
Total Flow- Using the "Magic Box"
Tank Duration
Alveolar Air Equation
P(A-a)O2 Gradient
Arterial & Venous O2 Content
Heliox Flow Rates
Body Humidity
Aerosolized Drug Administration
Aerosolized medications have been used for centuries
to treat respiratory diseases. Until recently, inhalation therapy
focused primarily on the treatment of asthma and chronic obstructive
pulmonary disease, and the pressurized metered-dose inhaler
was the delivery device of choice. However, the role
of aerosol therapy is clearly expanding beyond that initial
focus. This expansion has been driven by the
Montreal protocol and the need
to eliminate chlorofluorocarbons (CFCs) from traditional metered-dose
inhalers, by the need for delivery devices and
formulations that can efficiently and reproducibly target the
systemic circulation for the delivery of proteins and peptides,
and by developments in medicine that have made it possible to
consider curing lung diseases with aerosolized gene therapy
and preventing epidemics of influenza and measles with aerosolized
vaccines.
Each of these drivers has contributed to a decade or more of
unprecedented research and innovation that has altered how we
think about aerosol delivery and has expanded the role of aerosol
therapy into the fields of systemic drug delivery, gene therapy,
and vaccination. During this decade of innovation, we have witnessed
the coming of age of dry powder
inhalers, the development of new soft mist inhalers, and improved
pressurized metered-dose inhaler delivery as a result of the
replacement of CFC propellants with hydrofluoroalkane. The
continued expansion of the role of aerosol therapy will probably
depend on demonstration of the safety of this route of administration
for drugs that have their targets outside the lung and are administered
long term (eg, insulin aerosol), on the development of new drugs
and drug carriers that can efficiently target hard-toreach cell
populations within the lungs of patients with disease (eg, patients
with cystic fibrosis or lung cancer), and on the development
of devices that improve aerosol delivery to infants, so that
early intervention in disease processes with aerosol therapy
has a high probability of success.(The
Expanding Role of Aerosols in Systemic Drug Delivery, Gene Therapy,
and Vaccination Beth L Laube PhD)http://www.rcjournal.com/contents/09.05/09.05.1161.pdf
Nebulizer Designs Design differences among pneumatically powered, small-volume
nebulizers affect drug disposition (percentage of the dose delivered
to the patient, lost to deposition in the equipment, and lost
via
exhalation to ambient air) and thus affect drug availability
and efficacy. (Performance Comparison of Nebulizer Designs:
Constant-Output, Breath-Enhanced, and Dosimetric Joseph L Rau
PhD RRT FAARC, Arzu Ari MSc CRT CPFT, and Ruben D Restrepo MD
RRT) http://www.rcjournal.com/contents/02.04/02.04.0174.pdf
Constant-Output Nebulizers Constant output designs are the most commonly used
nebulizers, however they have been criticized as unreliable
and inefficient, because a low percentage of the dose reaches
the patient. The nebulizer provides aerosol at a fairly constant
rate during both inspiration and expiration.
B reath-Enhanced Nebulizers Breath-enhanced nebulizers
work by allowing air inhaled by the patient to be drawn through
the nebulizer which enhances the rate of air and aerosol output
from the nebulizer during inspiration. During
expiration the nebulizer falls back to a lower rate of aerosol
delivery. Droplet size is claimed to be more "stable"
or constant as compared to constant-ourput nebulizers.
Dosimetric Nebulizers Dosimetric or "breath
actuated" release aerosol during inspiration only.
During exhalation or when the patient holds their breath the
dosimetric does not release aerosol.
MDI Drug Administration
Inhaled medications are the main therapy for bronchial asthma
and chronic obstructive pulmonary disease (COPD). The major
advantage of inhaled therapy is that medications are delivered
directly into the airways, which
produces a high local concentration with significantly less
risk of systemic adverse effects. Poor
handling and inhalation technique are associated with decreased
medication delivery and poor disease control. Different
types of inhalers are available. Pressurized metered-dose inhaler
(MDI) was the earliest device and is the most commonly used
one. MDIs are difficult to use, have a high rate of incorrect
handling (7–71%), and require patient-device coordination.
(Handling of Inhaler Devices in Actual Pulmonary Practice:
Metered-Dose Inhaler Versus Dry Powder Inhalers) http://www.rcjournal.com/contents/03.08/03.08.0324.pdf
The use MDI's by patients incorrectly has led to a number
of studies and reccomendations to improve use and drug delivery.
Respiratory Therapists play a vital role in assuring that patients
are prorperly instucted in the use and function of MDI delivery
devises. (Instruction of Hospitalized Patients by Respiratory
Therapists on Metered-Dose Inhaler Use Leads to Decrease in
Patient Errors)ttp://www.rcjournal.com/contents/08.05/08.05.1040.pdf
Many inhaled medications currently used for asthma
are available in MDIs. Historically, MDI technology has utilized
chlorofluorocarbons (CFCs) as propellants. CFCs usually constitute
95 percent or more of the formulation emitted from an MDI. CFCs
are metabolically stable, and even the portion of an actuation
that is systemically absorbed is quickly excreted unchanged
via exhalation. CFCs have been
found to deplete stratospheric ozone, however, and have been
banned internationally. Although a temporary
medical exemption has been granted, it is expected that MDIs
with CFC propellant will be phased out completely. For example,
albuterol CFC will be phased out by the end of 2008. Alternatives
include MDIs with other propellants (nonchlorinated propellants
such as HFA 134a do not have ozone-depleting properties); multidose,
breath-activated DPIs; and other handheld devices with convenience
and delivery characteristics similar to current MDIs. MDIs with
HFA 134a have been approved for use with albuterol, levalbuterol,
beclomethasone dipropionate, and fluticasone propionate. Additional
non-CFC products and delivery systems are expected in the future.
Albuterol MDIs with HFA propellant deliver comparable doses
to the lung and produce comparable efficacy and safety as albuterol
CFC-MDIs. Beclomethasone dipropionate with HFA propellant delivers
a significantly greater dose to the lungs than its respective
CFC-MDIs, however, resulting in lower recommended doses, whereas
fluticasone propionate with HFA propellant delivers slightly
less drug to the lungs than the CFC-MDI but dosage recommendations
are unchanged. During the phaseout of CFC products, clinicians
will need to be informed of the alternatives and assist their
patients in the transition to non-CFC products. http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.pdf
I t is widely recognized that patients
frequently make mistakes when using their MDIs.
In one large study, 78% of the patients made an error
during MDI use.7 The 2 most common errors were failure to exhale
appropriately before actuation, and uncoordinated actuation
and inhalation. MDI errors are made by males and females, older
and younger adults, and patients with asthma and chronic obstructive
pulmonary disease (COPD).8 Similar errors are seen with children.
During asthma exacerbations, 75% of children made at least one
MDI error, and 45% made multiple errors. (Getting Back to
the Basics: Administering Inhaled Bronchodilators) http://www.rcjournal.com/contents/04.09/04.09.0455.pdf
Inhaled aerosol drugs commonly used by patients with chronic
obstructive pulmonary disease include short-acting and long-acting
bronchodilators, as well as corticosteroids. These agents are
available in a variety of inhaler devices, which include metered-dose
inhalers (MDI), breathactuated MDIs, nebulizers, and, currently,
5 different models of dry powder inhaler (DPI). There is evidence
to suggest that multiple inhaler types cause confusion among
patients and increase errors in patient use. Problems with MDIs
include failure to coordinate inhalation with actuation of the
MDI, inadequate breath-hold, and inappropriately fast inspiratory
flow. Lack of a dose
counter makes determining the number of remaining doses in an
MDI problematic. Patient misuse of MDIs is compounded by lack
of knowledge of correct use among health-care professionals.
Several factors often seen with elderly patients have been identified
as predictive of incorrect use of MDIs. These include mental-state
scores, hand strength, and ideomotor dyspraxia.
Holding chambers and spacers are partially intended to reduce
the need for inhalation-actuation coordination with MDI use.
However, such add-on devices can be subject to incorrect assembly.
Possible delays between MDI actuation and inhalation, rapid
inspiration, chamber electrostatic charge, and firing multiple
puffs into the chamber can all reduce the availability of inhaled
drug. Because they are breath-actuated, DPIs remove the need
for inhalation-actuation synchrony, but there is evidence that
patient errors in use of DPIs may be similar to those with MDIs.
One of the biggest problems is loading and priming the DPI for
use, and this may be due to the fact that every DPI model in
current use is different. Medical personnel’s knowledge
of correct DPI use has also been shown to be lacking. The optimum
inhalation profiles are different for the various DPIs, but,
generally, chronic obstructive pulmonary disease patients have
been shown to achieve a minimum (Practical Problems With Aerosol Therapy in COPD Joseph
L Rau PhD RRT FAARC) http://www.rcjournal.com/contents/02.06/02.06.0158.pdf
Chest Physiotherapy
The conventional method of CPT is chest percussion, which is
often accompanied by postural drainage. Chest percussion is
the manual pounding or clapping to loosen secretions. Postural
drainage relates to the positioning of a person to drain and
remove secretions from particular areas of the lungs. The specific
positions involved in postural drainage allow different
Chest physical therapy (CPT) is a widely used intervention for
patients with airway diseases. The main goal is to facilitate
secretion transport and thereby decrease secretion retention
in the airways. Historically, conventional CPT has consisted
of a combination of forced expirations (directed cough or huff),
postural drainage, percussion, and/or shaking. CPT improves
mucus transport, but it is not entirely clear which groups of
patients benefit from which CPT modalities. In general, the
patients who benefit most from CPT are those with airways disease
and objective signs of secretion retention (eg, persistent rhonchi
or decreased breath sounds) or subjective signs of difficulty
expectorating sputum, and with progression of disease that might
be due to secretion retention (eg, recurrent exacerbations,
infections, or a fast decline in pulmonary function).
The most effective and important part of conventional CPT is
directed cough. The other components of conventional CPT add
little if any benefit and should not be used routinely. Alternative
airway clearance modalities (eg, high-frequency chest wall compression,
vibratory positive expiratory pressure, and exercise) are not
proven to be more effective than conventional CPT and usually
add little benefit to conventional CPT. Only if cough and huff
are insufficiently effective should other CPT modalities be
considered. The choice between the CPT alternatives mainly depends
on patient preference and the individual patient’s response
to treatment. (Conventional Chest Physical Therapy for Obstructive Lung
Disease: Cees P van der Schans PT PhD)http://www.rcjournal.com/contents/09.07/09.07.1198.pdf
Postural Drainage Postural Drainage involves a patient assuming various
positions to facilitate the flow of secretions from various
parts of the lung into the bronchi, trachea and throat so that
they can be cleared and expelled from the lungs more easily.
The diagram below shows the correct positions to assume for
draining different parts of the lung.
Incentive Spirometry AARC
Clinical Practice Guideline for SMI
Incentive spirometry is designed to mimic natural sighing or
yawning by encouraging the patient to take long, slow, deep
breaths. This is accomplished by using a device that provides
patients with visual or other positive feedback when they inhale
at a predetermined flowrate or volume and sustain the inflation
for a minimum of 3 seconds.The objectives of this procedure
are to increase transpulmonary pressure and inspiratory volumes,
improve inspiratory muscle performance, and re-establish or
simulate the normal pattern of pulmonary hyperinflation. When
the procedure is repeated on a regular basis, airway patency
may be maintained and lung atelectasis prevented and reversed.
Positive Expiratory Pressure
(PEP Therapy)
Positive expiratory pressure (PEP) breathing is a form of chest
physiotherapy in which the patient
expires against a resistance. There are 2 conceptually
different methods to apply PEP: threshold resistor devices,
and flow resistor devices. The PEP mask (a flow resistor device)
was developed in Denmark in the late 1970s, and it soon became
a popular treatment in Scandinavia, Europe, and Canada. With
the PEP mask, the magnitude of the expiratory pressure is determined
by airflow and by the applied outflow resistor. The PEP mask
is thus a flow resistor device. At a constant expiratory flow,
the outflow resistance is inversely correlated to the diameter
of the outflow resistor. PEP is also related to airflow. With
a given outflow resistor, an increase in flow increases PEP,
and a decrease in flow decreases PEP. (Physiological Responses
to Positive Expiratory Pressure Breathing: A Comparison of the
PEP Bottle and the PEP Mask)http://www.rcjournal.com/contents/08.07/08.07.1000.pdf
Positive-expiratorypressure mask
physiotherapy (mask PEP) consists of cycles of active breathing
through a face mask against an expiratory resister. Mask
PEP, as with any airway-clearance technique, might ideally suit
the needs of patients with mild-to-moderate airway obstruction,
but it might not be equally suitable and effective for patients
with CF and severe airway obstruction. (Chest Physiotherapy
With Positive Airway Pressure: A Pilot Study of Short-Term Effects
on Sputum Clearance in Patients With Cystic Fibrosis and Severe
Airway Obstruction)http://www.rcjournal.com/contents/10.06/10.06.1145.pdf
IPPB involves applying the application of inspiratory positive
pressues to the airways. It typically is accompanied by the
administration of an aerosol with a bronchodialator.
IPPB has a past history of over-utilization coupled with a lack
of scientific evidence to support its use. However,
IPPB can be helpful if targeted towards specific conditions
that require airwary recuritment in individuals who lack the
ability to increase their resting volumes on their own. Patient's
with atlectasis with reduce vital capacites in the post-operative
stage may benefit from the positive pressure and airway recruitment
of IPPB. Proper application of the procedure is critical to
improve patient outcomes. Mis-application of IPPB can result
in poor outcomes and failure ot achieve patient goals. As with
the applicaiton of any presure applied to patient airways, proper
monitoring of delivered tidal volumes and pressures are imprtant
to limit any complications associated with baratrauma or volutrauma.
Trouble-Shooting: Common IPPB Problems
1. Will not cycle from inspiration to expiration:
-(LEAK) in the circuit or at patient (mouth seal).
2. Will not cycle on to inspiration:
-Sensitvity not set correctly
-Flow not turned on
3. Machine Auto-Cycles
- Sensitivity set to "sensitive
- Expiratory timer turned on
Partial List of Indications/Contraindications & Complications:
Refer to the AARC
CPG: IPPB for Complete Listings
Indications
Hypoventilation Atelectasis Contraindications:
Untreated Pneumothorax
Hemodynamic instability
Active TB Complications
Hyperventilation (common)
Decreased Cardiac Output (Venous Return)
Barotrauma
Gastric Insufflation
High-Frequency Chest Compression
"High-frequency chest-wall compression (HFCWC) is an established
therapeutic adjunct for patients with chronic pulmonary disorders
that impair bronchopulmonary secretion clearance. High-frequency
chest-wall compression (HFCWC) applies rapid but gentle external
compressions to the thorax to generate air flow velocities that
facilitate bronchopulmonary secretion clearance.
HFCWC is typically delivered in a timed, standardized fashion,
with a vest attached to an air-pulse generator."
(High-Frequency Chest-Wall Compression During the 48 Hours Following
Thoracic Surgery)James S Allan MD FAARC, Julie M Garrity
BSN, and Dean M Donahue MD
Deep Breathing &
Clearence Techniques
"The normal mechanism for lung expansion and bronchial
hygiene is spontaneous deep breathing (including yawn and sigh
maneuvers) and an effective cough. Instructing and encouraging
the patient to take sustained deep breaths is among the safest,
most effective, and least expensive strategies for keeping the
lungs expanded and secretions moving.9 A deep breath is a key
component of a normal effective cough. The negative intrathoracic
pressure enerated during spontaneous deep breathing tends to
better inflate the less compliant, gravity-dependent areas of
the lung than do methods that rely on lung inflation by application
of positive airway pressure. An effective cough is a vital component
of bronchial hygiene therapy." (Forced
Expiratory Technique, Directed Cough, and Autogenic Drainage)James B Fink MSc RRT FAARC.
-Forced Expiratory Technique
-Active Cycle of Breathing Technique
-Autogenic Drainage
The principle of pulse oximetry is based on the red and infrared
light absorption characteristics of oxygenated and deoxygenated
hemoglobin. Oxygenated hemoglobin absorbs more infrared light
and allows more red light to pass through. Deoxygenated (or
reduced) hemoglobin absorbs more red light and allows more infrared
light to pass through. Red light is in the 600-750 nm wavelength
light band. Infrared light is in the 850-1000 nm wavelength
light band.
Pulse oximetry uses a light emitter with red and infrared LEDs
that shines through a reasonably translucent site with good
blood flow. Typical adult/pediatric sites are the finger, toe,
pinna (top) or lobe of the ear. Infant sites are the foot or
palm of the hand and the big toe or thumb. Opposite the emitter
is a photodetector that receives the light that passes through
the measuring site.
There are two methods of sending light through the measuring
site: transmission and reflectance. In the transmission method,
as shown in the figure on the previous page, the emitter and
photodetector are opposite of each other with the measuring
site in-between. The light can then pass through the site. In
the reflectance method, the emitter and photodetector are next
to each other on top the measuring site. The light bounces from
the emitter to the detector across the site. The transmission
method is the most common type used and for this discussion
the transmission method will be implied. After the transmitted
red (R) and infrared (IR) signals pass through the measuring
site and are received at the photodetector, the R/IR ratio is
calculated. The R/IR is compared to a "look-up" table
(made up of empirical formulas) that convert the ratio to an
SpO2 value. Most manufacturers have their own look-up tables
based on calibration curves derived from healthy subjects at
various SpO2 levels. Typically a R/IR ratio of 0.5 equates to
approximately 100% SpO2, a ratio of 1.0 to approximately 82%
SpO2, while a ratio of 2.0 equates to 0% SpO2.
The major change that occurred from the 8-wavelength Hewlett
Packard oximeters of the '70s to the oximeters of today was
the inclusion of arterial pulsation to differentiate the light
absorption in the measuring site due to skin, tissue and venous
blood from that of arterial blood. At the measuring site there
are constant light absorbers that are always present. They are
skin, tissue, venous blood, and the arterial blood. However,
with each heart beat the heart contracts and there is a surge
of arterial blood, which momentarily increases arterial blood
volume across the measuring site. This results in more light
absorption during the surge. If light signals received at the
photodetector are looked at 'as a waveform', there should be
peaks with each heartbeat and troughs between heartbeats. If
the light absorption at the trough (which should include all
the constant absorbers) is subtracted from the light absorption
at the peak then, in theory, the resultants are the absorption
characteristics due to added volume of blood only; which is
arterial. Since peaks occur with each heartbeat or pulse, the
term "pulse oximetry" was coined. This solved many
problems inherent to oximetry measurements in the past and is
the method used today in conventional pulse oximetry.
Still, conventional pulse oximetry accuracy suffered greatly
during motion and low perfusion and made it difficult to depend
on when making medical decisions. Arterial blood gas tests have
been and continue to be commonly used to supplement or validate
pulse oximeter readings. The advent of "Next Generation"
pulse oximetry technology has demonstrated significant improvement
in the ability to read through motion and low perfusion; thus
making pulse oximetry more dependable to base medical decisions
on. http://www.oximeter.org/pulseox/principles.htm
Arterial blood gases are drawn to help assess acid/base balance
and as a tool for oygenation assessment. Typical sites for access
are the radial, brachial and femoral arteries. The radial is
the preferable site due to its ease of access. Universal precautions
should be used when drawing blood products and aseptic technique
is important in preventing contamination to the patient. Gloves
serve as an important barrier to blood contamination and eye
protection is also important when working with blood products.
Proper technique is important in both obtaining the sample and
preventing any complications from the procedure.
The use of the Modified Allen's
Test helps assure adequate collateral circulation
is present prior to the radial arterial stick. To perform the
test occlude both the radial and ulner arteries using your index
fingers. Make sure you hold the patient's arm higher then the
levle of their heart and have open and close their hands several
times. Release the pressure on the ulnar artery. The hand should
flush with blood indicating adequate collateral circulation
is present.
Arterial Blood Gas Analysis
Arterial blood is drawn and then analyzed to measure common
values such as : PH, PaCO2, PaO2, O2Sat. In addition ABG machines
are able to measure hemogloin vaiants (HBCO MetHB) and certain
electrolyte levels. The newer generation machines have the capability
to measure other values such as blood glucose and other metabolites.
Blood gas machines must maintain quality control standards to
assure accuray. Machine have built in quality control routines
suc as a“one-point calibration” is an adjustment
of the electronic response of an electrode to a single standard.
External controls are also run to assure accuracy and to maintain
lab certification requirements and standards.
At one time, it is was reccomend standard that all arterial
blood gas samples be placed on ice prior to measurment and immediatley
after collection. The theory was that any delay in measurement
could alter the accuracy of the results since oxygen would be
continued to be consumed under normal metabolic conditions.
Subsequently, placing the sample on ice was believed to slow
down the oxygen consumption and maintain sample accuracy. Reccent
guidelines contradict this previous practice and reccomend that
samples not be placed on ice unless certain conditions exist.
According to the AARC CPG for
ABG Sampling: Specimens held at room temperature must be analyzed
within 10-15 minutes of drawing; iced samples
should be analyzed within 1 hour.' The PaO2 of samples drawn
from subjects with elevated white cell counts may decrease very
rapidly. Immediate chilling is necessary. Some dual-purpose
electrolyte/blood gas analyzers stipulate immediate analysis
without chilling because of possible elevations in potassium
from chilling; however, the accuracy of the blood gas results
should not be affected by the chilling.
Arterial Line Placement Method: Usually placed on the
inner side of the wrist. It could also be placed in the artery
on the inner side of the elbow, the groin or the foot.
The area is decided mainly upon how well
your pulse is felt. That area of the skin cleaned well with
a disinfecting solution and alcohol. Then, the pulse is felt.
With a small needle the skin is numbed with local anesthesia.
Then, using a needle with a plastic catheter the skin is entered.
Once inside the artery, the plastic catheter is advanced further
in and the needle is removed. The catheter is then connected
to some tubing. The are is then covered with a bandage.
A blood sample obtained from a heel puncture and finger prick
is a useful and simple way of collecting blood samples. It can be used to monitor:
-Blood glucose levels
-Drug levels -Blood gases
-Full blood counts
-Urea and electrolytes
-Newborn Bloodspot Screening Tests The procedure is not without risk. The main problems are:
-Increased pain
-Local trauma
-Damage to nerves, blood vessels and bones
-Excessive blood loss
-Infection Heel
& Finger Puncture Techniques
"Transcutaneous monitoring measures skin-surface PO2 and
PCO2 to provide estimates of arterial partial pressure of oxygen
and carbon dioxide (PaO2 and PaCO2). The devices induce hyperperfusion
by local heating of the skin and measure the partial pressure
of oxygen and carbon dioxide electrochemically. PtcO2 is an
indirect measurement of PaO2 and, like PaO2, does not reflect
oxygen delivery or oxygen content. Complete assessment of oxygen
delivery requires knowledge of hemoglobin, saturation, and cardiac
output. In a similar way, PtcCO2 is an indirect measurement
of PaCO2 but knowledge of delivery and content is not necessary
to use PtcCO2 as an indicator of adequacy of ventilation."
National
Guideline Clearinghouse
"Capnography is a simple
method of monitoring the concentration or partial pressure of
carbon dioxide (CO2) in the respiratory gases.
The fundamentals of capnography use were established in 1943
by Luft who discovered that CO2 could absorb infrared (IR) radiation.
Capnography was first used in Holland in 1978, and subsequently
its usefulness was approved for monitoring during anesthesia.
Nowadays, capnography is a standard of care for monitoring patient
safety in anesthesia, but it has not yet been accepted for routine
use in emergency department procedural sedation and analgesia.
Several procedures are available for monitoring airway CO2.
The first procedure is by using a side stream sample measured
through a rapidly responding infrared CO2 analyzer or measured
through a mass spectrometer. The second procedure is direct
measurement of CO2 values through an infrared analyzer at the
end of the endotracheal tube. These procedures correspond to
the term capnography or airway CO2 monitoring.
Capnography is a graphic display
of CO2 concentration during the respiratory cycle,
while capnometry is a numerical display of CO2 concentration
during the respiratory cycle. This method of monitoring directly
shows the elimination of CO2 by the lungs and indirectly reflects
the production of CO2 by tissues and CO2 circulatory transport
to the lungs. Capnography is a non-invasive and accurate method.
The need for arterial blood sampling can be significantly reduced.
Capnography directly measures the ventilatory performance of
the lungs and indirectly presents measurements on the performance
of metabolism and circulation. An important use of capnography
is as a non-invasive assessor of proper endotracheal tube placement.
An advantage of capnography is
that it provides an immediate picture of patient apnea, while
pulse oximetry is delayed for several minutes." Clinical
Applications of Capnography
Indirect calorimetry
measures resting metabolic rate, or the number of calories your
body burns at rest. It
can also measure how many calories your body burns after eating.
The test involves measuring the amount of oxygen
a subject breathes in, and the amount of carbon dioxide (CO2)
breathed out. From these gas exchange data, the number of calories
burned per minute is determined. Metabolic
measurements using indirect calorimetry for determination of
oxygen consumption (VO2), carbon dioxide production (VCO2),
respiratory quotient (RQ), and resting energy expenditure (REE)
as an aid to patient nutritional assessment and management;
assessment of weaning success and outcome; assessment of the
relationship between O2 delivery (DO2) and VO2; and assessment
of the contribution of metabolism to ventilation. The guideline
addresses metabolic measurement during mechanical ventilation.
Metabolic measurements use an indirect calorimeter to measure
VO2 and VCO2 via expired gas analysis. The measurements of VO2
and VCO2 are used to calculate RQ (VCO2/VO2) and REE using the
Weir equation: REE = [VO2 (3.941) + VCO2 (1.11)] 1440 min/day.
National
Guideline Clearinghouse
Cardiac Strees Testing
& Analysis "Cardiovascular
(heart and blood vessel) disease is the leading cause of death
in developed nations. Assessing the heart's function and examining
the seriousness of coronary artery (the blood vessels of the
heart) disease are the goals of cardiac stress testing. Putting
stress on the heart, such as with exercise or certain medications,
makes the heart work harder. Under these conditions, myocardial
ischemia (diminished blood flow to the heart muscle) may occur.
As part of an evaluation for cardiovascular disease in someone
with chest pain (in addition to an electrocardiogram [ECG]),
cardiac stress testing may be helpful in determining the need
for invasive tests such as coronary angiography—visualizing
coronary arteries after injecting dye through a cardiac catheter
(tube inserted into the heart). The October 15, 2008, issue
of JAMA includes an article about cardiac stress testing.
Exercise stress tests use cardiac
monitoring while an individual walks on a treadmill with an
increasingly steep incline. Technicians measure the heart rate,
time walked on the treadmill, and the effort during the test,
and the doctor looks for ECG changes. Nuclear stress tests use
an injection of a radionuclide (a compound with a slight amount
of radioactivity) to track blood flow and the pattern of ischemia
when the heart is stressed (either with exercise or with medication).
Pharmacologic stress tests, often used for persons who cannot
walk for more than a short distance, use drugs that put stress
on the heart muscle. ECG and other cardiac monitors record data,
including heart rate and rhythm. Changes in the ECG and/or cardiac
imaging may indicate ischemia. Echocardiography (using sound
waves to look at heart structures and at blood flow in the heart's
chambers) can be combined with stress testing to examine the
function of the heart at rest and under stress conditions. "
JAMA
Reference SiteJAMA
- Cardiac Strees Testing Overview
ECG Monitoring &
Interpretation
The
ECG is a recording of the electrical activity of the heart.
It does not provide information about the mechanical function
of the heart and cannot be used to assess cardiac output or
blood pressure. A good electrical connection between the patient
and the electrodes is required to minimise the resistance of
the skin. For this reason gel pads or suction caps with electrode
jelly are used to connect the electrodes to the patients skin.
However when the skin is sweaty the electrodes may not stick
well, resulting in an unstable trace. An electrical
recording made from one myocardial muscle cell will record an
action potential (the electrical activity which occurs when
the cell is stimulated). The ECG records the vector sum (the
combination of all electrical signals) of all the action potentials
of the myocardium and produces a combined trace.
The Sinoatrial (SA) node, internodal pathways, Atrioventricular
(AV) node, bundle of HIS with right and left bundle branches
and the Purkinje system. The left bundle branch also divides
into anterior and posterior fascicles. Conducting tissue is
made up of modified cardiac muscle cells which have the property
of automaticity, that is they can generate their own intrinsic
action potentials as well as responding to stimulation from
adjacent cells. The conducting pathways within the heart are
responsible for the organised spread of action potentials within
the heart and the resulting co-ordinated contraction of both
atria and ventricles.
* The P - R Interval is taken from the
start af the P wave to the start of the QRS complex. It is the
time taken for depolarisation to pass from the SA node via the
atria, AV node and His-Purkinje system to the ventricles.
* The QRS represents the time taken for depolarisationto pass
through the His-Purkinje system and the ventricular muscles.
It is prolonged with disease of the His-Purkinje system.
* The Q - T interval is taken from the start of the QRS complex
to the end of the T wave. This represents the time taken to
depolarise and repolarise the ventricles.
* The S - T segment is the period between the end of the QRS
complex and the start of the T wave. All cells are normally
depolarised during this phase. The ST segment is changed by
pathology such as myocardial ischaemia or pericarditis.
The ECG may be used in two ways. A 12 lead ECG may be performed
which analyses the cardiac electrical activity from a number
of electrodes positioned on the limbs and across the chest.
A wide range of abnormalities may be detected including arrhythmias,
myocardial ischaemia, left ventricular hypertrophy and pericarditis.
The ECG may be used in two ways. A 12 lead ECG may be performed
which analyses the cardiac electrical activity from a number
of electrodes positioned on the limbs and across the chest.
A wide range of abnormalities may be detected including arrhythmias,
myocardial ischaemia, left ventricular hypertrophy and pericarditis.
* Lead I - measures the potential difference between the right
arm electrode and the left arm electrode. The third electrode
(left leg) acts as neutral.
* Lead II - measures the potential difference between the right
arm and left leg electrode.
* Lead III - measures the potential difference between the left
arm and left leg electrode.
"Polysomnography
is a multi-parametric test that is used to study/record in detail
all the biophysiological changes that occur in the human body
when the person is asleep. The PSG or polysomnogram,
as the test is referred to, measures or monitors many body functions
including the eye movements (EOG), brain (EEG), heart rhythm
(ECG), skeletal muscle activation (EMG), and breathing or respiratory
effort during sleep, and based on the observations, the doctor
will decide whether the person who had undergone PSG suffers
from obstructive sleep apnea (OSA) or any of its namesakes or
not. Even though PSG can be done at any time, usually it is
performed at night when everybody usually sleeps except in certain
special cases when the tests are done over two days time.
Of the eleven channels, two
are for EEG - to determine if the person is indeed sleeping
and in what stage of sleep he/she is at a given time - one
channel to measure air flow, one channel each to sense chin
and leg movements, two channels to measure REM, one channel
each for EKG and oxygen saturation, and one for recording the
chest and abdominal wall movements. All these
channels are then wired to a computer where it is deciphered
into readable attributes and stored for future reference or
record. A live video of the sleeping patient is also recorded
so that the supervising technician could observe the patient
from an adjacent room. The same clips may also be used by the
doctor for further diagnosis of the patient. Despite all the
wires attached to the patient, interestingly, it has been found
that few patients ever have any problems sleeping whilst under
observation. Most of them stated they even slept better in the
lab than at home." Polysomnography
Reference Site
"The objective of spirometry is to assess ventilatory function.
Spirometry includes but is not limited to the measurement of forced
vital capacity (FVC), the forced expiratory volume in the first
second (FEV1), and other forced expiratory flow measurements such
as the FEF25-75%. In addition, it sometimes includes the measurement
of maximum voluntary ventilation (MVV). A graphic representation
(spirogram) of the maneuver should be a part of the results. Either
a volume-time or flow-volume display is acceptable. Other parameters
that may be obtained by spirometry include FEFmax (PEF), FEF75%,
FEF50%, FEF25%, FIF50%, and FIFmax (PIF). "
"Spirometry is an effort-dependent test that requires
careful instruction and the cooperation of the test subject.
Inability to perform acceptable maneuvers may be due to poor
subject motivation or failure to understand instructions. Physical
impairment and young age (eg, children < 5 years of age)
may also limit the subject's ability to perform spirometric
maneuvers. These limitations do not preclude attempting spirometry
but should be noted and taken into consideration when the results
are interpreted."
Forced Expiratory Volume in
1 Second
The FEV1 is the most widely used parameter to measure the mechanical
properties of the lungs. In normal persons, the FEV1 accounts
for the greatest part of the exhaled volume from a spirometric
maneuver and reflects mechanical properties of the large and
the medium-sized airways. In a normal flow-volume loop, the
FEV1 occurs at about 75% to 85% of the FVC. This parameter is
reduced in obstructive and restrictive disorders. In obstructive
diseases, FEV1 is reduced disproportionately to the FVC, reducing
the FEV1/FVC ratio below the lower limit of normal and indicates
airflow limitation. In restrictive disorders, the FEV1, FVC,
and total lung capacity are all reduced, and the FEV1/FVC ratio
is normal or even elevated.
Forced Vital Capacity
FVC is a measure of lung volume and is usually reduced in diseases
that cause the lungs to be smaller. Such processes are generally
termed restrictive and can include disorders of the lung parenchyma,
such as pulmonary fibrosis, or of the bellows, including kyphoscoliosis,
neuromuscular disease, and pleural effusion. However, a reduction
in FVC is not always due to reduced total volumes and can occur
in the setting of large lungs hyperinflated due to severe airflow
obstruction and air trapping, as in emphysema. In this setting,
the FVC is decreased due to reduced airflow, air trapping, and
increased residual volume, a phenomenon referred to as pseudorestriction.
Reduced FVC can occur despite a normal or increased total lung
volume. Therefore, FVC is not a reliable indicator of total
lung capacity or restriction, especially in the setting of airflow
obstruction. The overall accuracy of the FVC for restriction
is about 60%. 5
"The results of spirometry should meet the following criteria
for number of trials, acceptability, and reproducibility. The
acceptability criteria should be applied before reproducibility
is checked. Number of trials: A minimum of 3 acceptable FVC
maneuvers should be performed. If a subject is unable to perform
a single acceptable maneuver after 8 attempts, testing may be
discontinued. However, after additional instruction and demonstration,
more maneuvers may be performed depending on the subject's clinical
condition and tolerance.
Acceptability: A good 'start-of-test' includes:
A an extrapolated volume of < or = 5% of the FVC or 150 mL,
whichever is greater;
No hesitation or false start;
A a rapid start to rise time.
Acceptability: no cough, especially during the first second
of the maneuver.
Acceptability: no early termination of exhalation. "
"Chronic obstructive pulmonary disease is easily detected
in its preclinical phase, using office spirometry. Successful
smoking cessation prevents further disease progression in most
patients. Spirometry measures the ratio of the forced expiratory
volume in the first second to the forced vital capacity (FEV1/FVC),
which is the most sensitive and specific test for detecting
airflow limitation. Primary care practitioners see the majority
of adult smokers, but few primary care practitioners currently
have spirometers or regularly order spirometry for their smoker
patients. Improvements in spirometry software have made it much
easier to obtain good quality spirometry test sessions, thereby
reducing the misclassification rate. Respiratory therapists
and pulmonary function technologists can help primary care practitioners
select good office spirometers for identifying chronic obstructive
pulmonary disease and teach staff how to use spirometers correctly."
(Strategies
for Screening for Chronic Obstructive Pulmonary Disease)Paul L Enright MD and David A Kaminsky MD
Complete Pulmonary Function
Testing
Many of the current chronic obstructive pulmonary disease (COPD)
guidelines (eg, ATS-ERS and Global Obstructive Lung Disease
consortium [GOLD]) and asthma guidelines (Global Initiative
for Asthma [GINA]) recommend the FEV1/FVC ratio as the "gold
standard" to diagnose airway obstruction.
1. Assess flow and volume.
2. Forced vital capacity maneuver followed by forced inspiratory
vital capacity maneuver.
3. Flow rates are measured at 25%, 50% and 75% points. These
are know as Vmax flows.
4. Decrease in Vmax flow rates indicate obstruction.
5 Percent Predicted: Actua/Predicted = % predicted
6. Actual is derived from actual measurement Predicted is based
on a set standards derived from a person’s sex, age, height,
and weight.
Volume/Time & lung Volume
Graphs DLCO TESTING: Lung diffusion testing looks at how well gases
are passing from the air sacs of the lungs into the blood, to
determine whether the lung is sending enough oxygen into the
blood. The test measures the "diffusing capacity of the
lung for carbon monoxide" or DLCO. Measures limitation
of gas diffusion across alveolar capillary membrane. Measured
at STPD (standard temperature pressure dry). Single breath test
most widely used. Pt breaths 3% CO, 10% HE, and air holds their
breath for a minimum of 10 seconds. Normal value 25 ml/co/min/mmHg
at STPD. DLCO values increase 2-3x with exercise. A measurement
of alveolar volume (VA) is required for DLCO calculations because
it represents the gas volume into which CO is distributed and
then transferred across the alveolar capillary membrane. VA
is measured simultaneously with CO uptake by calculating the
dilution of an inert tracer gas and subtracting dead space volume.
DLCO is a general measure of the complete ‘efficiency'
of the lungs because it is influenced by three key components:
The surface area of the lung with contact to diffusing alveoli
(VA - Alveolar Volume), the thickness of the alveolar-capillary
membrane (Dm - Membrane Diffusion) and the volume of blood available
in the capillary bed of the lung (Vc - Capillary Blood Volume).
The CO is used to trace the diffusion in place of O2 because
it is a one-way transfer across the alveolar-capillary membrane
for combination with Hb. The helium in the mixture is used to
obtain a measure of the alveolar volume.
The challenge of Single Breath Diffusion testing is to obtain
a representative sample of gas from an area of the lungs where
diffusion is taking place. The patient first breathes all the
way out to residual volume and is then connected to the test
gas. They breathe all the way in to TLC and are then instructed
to hold their breath for approximately 10 seconds. After having
held your breath for ten seconds, the first amount of gas that
leaves your lips when you breathe out, has been resident in
the physiological dead-space (mouth, trachea and two main bronchi)
and must therefore be discarded before collecting a valid gas
sample.
DLCO values decreased in conditions associated with “alveolar
fibrosis”-
- asbestosis, sarcoidosis, O2 toxicity, edema etc.
DLCO is decreased in emphysema due to:
*decreased surface area for diffusion
*loss of capillary bed
*V/Q mismatch
LUNG VOLUMES:
"Understanding and identifying the lung volume components
is essential in pulmonary function testing. Measurements of
lung volumes are important to confirm or clarify the nature
of lung disorders. The flow volume loop may indicate an obstructive
or restrictive or obstructive/restrictive pattern, but a further
test of lung volume is often necessary for clarification. In
an obstructive lung disease, airway obstruction causes an increase
in resistance. During normal breathing, the pressure volume
relationship is no different from a normal lung. However, when
breathing rapidly, greater pressure is needed to overcome the
resistance to flow, and the volume of each breath gets smaller.
The increase in the effort to breathe can cause an overdistention
of the lungs.
The flow volume loop may show lower than normal FEV1 and FEF25-75,
but it is not until a lung volume has been determined that an
increase in TLC, FRC and RV can be confirmed. Common obstructive
disease include asthma, bronchitis and emphysema. In a restrictive
lung disease, the compliance of the lung is reduced which increases
the stiffness of the lung and limits expansion. In these cases,
a greater pressure than normal is required to give the same
increase in volume. The flow volume loop may show lower than
normal FVC, but the FEV1 and FEF25-75 may only be mildly effected.
The lung volume measurement will clearly show a reduction in
TLC, FRC and RV.
Tidal Volume (TV). The amount of gas inspired or expired with
each breath.
Inspiratory Reserve Volume (IRV). Maximum amount of additional
air that can be inspired from the end of a normal inspiration.
Expiratory Reserve Volume (ERV). The maximum volume of additional
air that can be expired from the end of a normal expiration.
Residual Volume (RV). The volume of air remaining in the lung
after a maximal expiration. This is the only lung volume which
cannot be measured with a spirometer.
Total Lung Capacity (TLC). The volume of air contained in the
lungs at the end of a maximal inspiration. Called a capacity
because it is the sum of the 4 basic lung volumes. TLC = RV+IRV+TV+ERV
Vital Capacity (VC). The maximum volume of air that can be forcefully
expelled from the lungs following a maximal inspiration. Called
a capacity because it is the sum of inspiratory reserve volume,
tidal volume, and expiratory reserve volume. VC = IRV+TV+ERV=TLC-RV
Functional Residual Capacity (FRC). The volume of air remaining
in the lung at the end of a normal expiration. Called a capacity
because it equals residual volume plus expiratory reserve volume.
FRC = RV+ERV
Inspiratory Capacity (IC). Maximum volume of air that can be
inspired from end expiratory position. Called a capacity because
it is the sum of tidal volume and inspiratory reserve volume.
This capacity is of less clinical significance than the other
three. IC = TV+IRV
BODY PLETHSMOGRAPHY:
(Body Box)
The body box calculates lung volumes in realtion to pressure
changes. Body plethysmography is the most accurate means available
at this time to assess lung volumes because it is not limited
by air trapping. If you have a closed container where volume
can be adjusted using a reciprocating pump (typically 30ml)
then the pressure in the container increases in amount proportional
to the fractional decrease in container volume (i.e. PV=k).
* The calculation is based on Boyle's Law:
o V1 P1 T1 = V2 P2 T2
For the plethysmograph, the temperature is kept constant so:
P1 V1 = P2 V2
Where:
P1 and V1 are initial pressure and volume.
P2 and V2 are final pressure and volume.
Note: Both measurements are made at a constant temperature.
To calibrate the box pressure signal, a 30ml sinusoidal pump
is used with the cabin door closed and the box sealed. The 30ml
stroke of volume in and out of the sealed box causes a change
in the box pressure signal. Thus the pressure change can be
calibrated against a known volume. In body plethysmography,
the patient sits inside an airtight box, inhales or exhales
to a particular volume (usually FRC), and then a shutter drops
across their breathing valve. The subject makes respiratory
efforts against the closed shutter causing their chest volume
to expand and decompressing the air in their lungs. The increase
in their chest volume slightly reduces the box volume and thus
increases the pressure in the box. This method of measuring
FRC actually measures all the conducting pathways including
abdominal gas; the actual measurement made is VTG (Volume of
Thoracic gas).
HELIUM DILUTION: During
helium dilution measurement of lung volumes, patients breathe
from a known volume and concentration of helium gas for a period
of typically 4 to 7 minutes. The oxygen concentration in the
starting mixture is set at 30% to ensure patients with COPD
can remain comfortable during the test. A carbon dioxide absorber
is situated in line with expired breath to keep the closed-circuit
CO2 level below 0.5% and avoid discomfort and hyperventilation.
Oxygen is added to the system to maintain the starting volume
in the spirometer.
Once connected to the closed-circuit, equilibration between
the starting and final helium concentrations should occur within
7 minutes. A state of equilibrium is defined as helium concentration
changes of less than 0.02% over a 30 second interval.The functional
residual capacity (FRC) is calculated from the helium concentrations
as follows:
FRC = (% helium initial - % helium final) / % helium final
x system volume
The dead space of the system (patient valve, filter and mouthpiece)
is subtracted from this value. The FRC can be underestimated
with the helium dilution technique in conditions such as bullous
emphysema or severe airways obstruction. Trapped lung gas does
not communicate with the inhaled helium mixture. Plethysmographic
measurement of lung volumes is preferred in these cases. The
FRC can be overestimated or unmeasurable when leaks are present.
Leaks may develop in the equipment valves or circuitry, or,
more commonly, at the mouthpiece. A system leak is likely to
be the cause if the graph of the delivered helium concentration
does not flatten, ie, when equilibrium is not reached, within
7 minutes.
http://www.morgansci.com/customer-resource-center/pulmonary-info-for-patients/what-is-a-pft-test-3.php
NITROGEN WASHOUT: Nitrogen
recovery is another gas dilution technique for measuring lung
volumes. Only those instruments that can measure DLCO can offer
N2 recovery ability. Since N2 is resident in the lung at all
times, it has an infinite time to reach whatever communicating
airways it can. During the performance of DLCO, the subject
exhales to residual volume (all the way empty) and then breathes-in
diffusion gas until completely full (TLC). The new N2 from the
DLCO mixture rapidly mixes with the N2 that was in the residual
volume and thus TLC can be directly measured. The technique
has to assume the partial pressure of CO2 in the alveolar at
the start of the test. For this reason, having a separate measure
of PACO2 (alveolar CO2) from an end-tidal CO2 monitor can greatly
improve accuracy on patients with COPD.
Bronchial
Provocation (Challenge) Testing "To define whether nonspecific airway hyperreactivity
is a mechanism for atypical chest symptoms of unclear origin,
inhalational challenge tests are often used in the pulmonary function
laboratory. Methacholine and histamine are the agents most often
used with this procedure, although other agents may also be useful.
Methacholine is considered safe, can be used in outpatient clinics,
and has no systemic side effects. Challenge testing determines
presence of airway hyper reactivity. After initial spirometry,
patient inhales a specific concentration of methacholine chloride
and spirometry is repeated. A reduction in FEV1 20% below the
prior test indicates asthma. When the baseline spirogram is relatively
normal, inhalational challenge may be performed by aerosolizing
progressive concentrations of methacholine by a dosimeter. This
is typically performed as a five-stage procedure with five different
increasing concentrations. After each stage, the patient performs
a spirometry. When there is a 20% reduction in the FEV1, the test
is terminated and is considered positive for airway hyperreactivity.
The provocative concentration dosage level of the inhalational
agent required to produce a 20% reduction in the FEV1 is labeled
PC20FEV1. If the drop in FEV1 is less than 20% after five stages
of this procedure, the challenge test is considered negative for
airway hyperreactivity. A PC20FEV1 of less than 8 mg/mL suggests
clinically important airway hyperreactivity.
When the baseline spirogram is relatively normal, inhalational
challenge may be performed by aerosolizing progressive concentrations
of methacholine by a dosimeter. This is typically performed as
a five-stage procedure with five different increasing concentrations.
After each stage, the patient performs a spirometry. When there
is a 20% reduction in the FEV1, the test is terminated and is
considered positive for airway hyperreactivity. The provocative
concentration dosage level of the inhalational agent required
to produce a 20% reduction in the FEV1 is labeled PC20FEV1. If
the drop in FEV1 is less than 20% after five stages of this procedure,
the challenge test is considered negative for airway hyperreactivity.
A PC20FEV1 of less than 8 mg/mL suggests clinically important
airway hyperreactivity." Cleveland
Clinic Information site
(An In Vitro Study to Investigate the Use of a Breath-Actuated,
Small-Volume, Pneumatic Nebulizer for the Delivery of Methacholine
Chloride Bronchoprovocation Agent) Jolyon P Mitchell
PhD C Chem, Mark W Nagel, Sara Lou Bates, and Cathy C Doyle
Exhaled
Nitric Oxide The measurement of exhaled nitric oxide as a reflection of
airway inflammation is gaining rapid acceptance as a pulmonary
function test. Normal values have been shown to depend on the
exhaled flow rate during the measurement. The test is repeated
until three reproducible results are obtained. The mean value
is reported. Patients are asked to inspire to total lung capacity
and then exhale into an analyzer using a steady, controlled exhaled
flow rate. The test is rapid and safe and can be performed by
most patients. The normal values shown in the Table below. Cleveland
Clinic Information site
PFT Quality Control Standards
Pulmonary function tests are most useful when performed with good
technique and with an accurate system. Using standard techniques
in performing the tests minimizes diagnostic and therapeutic errors.
This report
discusses the rationale and limits of standardization and offers
practical suggestions for using available standards to increase
confidence in test results. (Standards
and Interpretive Issues in Lung Function Testing) Robert O Crapo MD and Robert L Jensen PhD. "Diagnostic tests can only increase or decrease the
probability of the asthma diagnosis, so a thorough history is
very important. In patients with asthma-like symptoms, spirometric
evidence of airway obstruction plus a large bronchodilator response
makes asthma much more likely. However, normal spirometry is common
in patients with mild asthma who are not symptomatic at the time
of testing, and patients with poorly controlled asthma may lack
substantial bronchodilator response. Inhalation challenge test
often helps confirm asthma in patients with normal spirometry."
(Making
the Diagnosis of Asthma) Meredith C McCormack MD MHS and
Paul L Enright MD.
Pulmonary
Artery Catheter Line
While the PA catheter is inserted, the monitor will display
the various pressure waveforms associated with the catheter’s
position in the heart and vessels.
During the insertion procedure, the first waveform will be
the right atrial pressure. This wave will resemble a CVP wave.
The following waveform will be the right ventricular pressure
as the catheter passes through the right ventricle. During this
time, the patient may experience some ventricular dysrhythmias
that disappear as soon as the catheter exits the right ventricle.
The catheter will enter the pulmonary artery and this will be
its resting place for the majority of the time. Finally, when
the balloon is inflated, the catheter will float into the pulmonary
capillary and the resulting waveform will be the wedge pressure.
The proximal port, commonly termed the CVP port, is used to
measure right atrial or central venous pressure. It is also
used for medication infusion and fluid boluses for cardiac output
measurement.
The distal port is used for PA pressure measurements and PCWP
measurements when the balloon is inflated. Mixed venous blood
gases can also be drawn from this port. The balloon port which
is located at the tip of the catheter is inflated with a small
amount of air (less than 1.5cc). When inflated, this balloon
allows the catheter to float into a pulmonary artery branch
vessel. This is refered to as a wedge position. This position
allows pressure measurements to be made that indirectly reflect
left ventricular end diastolic pressure.
The thermistor port is connected to the patient’s monitor
via a cable and allows the display of continuous temperature
readings. These temperature readings are essential to calculate
cardiac output measurements. The actual thermistor is located
just proximal to the balloon. In order to determine the cardiac
output value, cool injectate is delivered rapidly through the
proximal port of the PA catheter. A temperature curve is plotted
over time as the cool injectate causes the pulmonary artery
temperature to fall. It then rises back to the previous core
temperature as warm blood continues in circulation.
Central Venous Pressure (CVP):
CVP readings are used to approximate the Right Ventricular End
Diastolic Pressure (RVEDP). The RVEDP assesses right ventricular
function and general fluid status.
o Low CVP values typically reflect hypovolemia or decreased
venous return.
o High CVP values reflect overhydration, increased venous return
or right sided cardiac failure.
Mean Arterial Pressure (MAP):
Reflects changes in the relationship between cardiac output
(CO) and systemic vascular resistance (SVR) and reflects the
arterial pressure in the vessels perfusing the organs.
o A low MAP indicates decreased blood flow through the organs.
o A high MAP indicates an increased cardiac workload.
Preload:
Preload occurs during diastole. It is the combination of pulmonary
blood filling the atria and the stretching of myocardial fibers.
Preload is regulated by the variability in intravascular volume.
o Volume reduction decreases preload
o Volume increase will increase preload, mean arterial pressure
(MAP) and stroke index (SI).
Pulmonary Artery Pressure (PA Pressure):
Blood pressure in the pulmonary artery.
o Increased pulmonary artery pressure may indicate: a left-to-right
cardiac shunt, pulmonary artery hypertension, COPD or emphysema,
pulmonary embolus, pulmonary edema, left ventricular failure.
Pulmonary Capillary Wedge Pressure (PCWP or PAWP):
PCWP pressures are used to approximate LVEDP (left ventricular
end diastolic pressure).
o High PCWP may indicate left ventricle failure, mitral valve
pathology, cardiac insufficiency, cardiac compression post hemorrhage.
Pulmonary Vascular Resistance (PVR):
The measurement of resistance or the impediment of the pulmonary
vascular bed to blood flow.
o An increased PVR or "Pulmonary Hypertension" is
caused by pulmonary vascular disease, pulmonary embolism, or
pulmonary vasculitis, or hypoxia.
o A decreased PVR is caused by medications such as calcium channel
blockers, aminophylline, or isoproterenol or by the delivery
of O2.
Right Ventricular Pressure (RV Pressure):
A direct measurement that indicates right ventricular function
and general fluid status.
o High RV pressure may indicate: pulmonary hypertension, right
ventricle failure, congestive heart failure.
Stroke Index or Stroke Volume Index: (SI or SVI):
The amount of blood ejected from the heart in one cardiac cycle,
relative to Body Surface Area (BSA). It is measured in ml per
meter square per beat.
o An increased SVI may be indicative of early septic shock,
hyperthermia, hypervolemia or be caused by medications such
as dopamine, dobutamine, or digitalis.
o A decreased SVI may be caused by CHF, late septic shock, beta
blockers, or an MI.
Stroke Volume (SV):
The amount of blood pumped by the heart per cardiac cycle. It
is measured in ml/beat.
o A decreased SV may indicate impaired cardiac contractility
or valve dysfunction and may result in heart failure.
o An increased SV may be caused by an increase in circulating
volume or an increase in inotropy.
Systemic Vascular Resistance (SVR):
The measurement of resistance or impediment of the systemic
vascular bed to blood flow.
o An increased SVR can be caused by vasoconstrictors, hypovolemia,
or late septic shock.
o A decreased SVR can be caused by early septic shock, vasodilators,
morphine, nitrates, or hypercarbia.
Formulas
Pulse Pressure = SAP Systolic - SAP Diastolic
M mean SAP = (SAP Systolic + 2*SAP Diastolic)/3
M ean PAP = (PAP Systolic + 2*PAP Diastolic)/3
SV Index = SV/BSA
Cardiac Output = (SV * HR) / 1000
Cardiac Index = CardiacOutput/BSA
BSA = (cm^0.718)*(kg^0.427)*0.007449
SVR = (meanSAP-meanRAP)*80/CardiacOutput
PVR = (meanPAP - Wedge Pressure)*80/CardiacOutput
Normal Values
SAP 100-140/60-90 mmHg
Mean SAP 70-100 mmHg
Pulse Pressure 30-50 mmHg
Heart Rate 60-100 bpm
RVP 17-30/0-6 mmHg
RAP 0-6 mmHg
Mean RAP 3 mmHg
PA Pressure 15-30/5-13 mmHg
Mean PA pressure 10-18 mmHg
Wedge Pressure 2-12 mmHg
SV 60-120 ml/contraction
SVI 40-5- ml/contraction/m^2
CO 3-7 L/min
CO index 2.5-4.5 L/min/m^2
SVR 800-1200 dynes/sec/cm^-5
PVR 120-250 dynes/sec/cm
Chest Tube Insertion
Drainage of the pleural space by means of a chest tube is
the commonest intervention in thoracic trauma, and provides
definitive treatment in the majority of cases. While a relatively
simple procedure, it carries a significant complication rate,
reported as between 2% and 10%. While many of these complications
are relatively minor, some require operative intervention and
deaths still occur.
Indications A chest tube is indicated to drain the contents
of the pleural space. Usually this will be air or blood, but
may include other fluids such as chyle or gastric/oesophageal
contents. Chest tube insertion is also appropriate to prevent
the development of a pleural collection, such as after a thoractomy
or to prevent a tension pneumothorax in the ventilated patient
with rib fractures.
Absolute Indications * Pneumothorax (tension, open or simple)
* Haemothorax
* Traumatic Arrest (bilateral)
Relative Indications * Rib fractures & Positive pressure ventilation
* Profound hypoxia / hypotension & penetrating chest injury
* Profound hypoxia / hypotension and unilateral signs to a hemithorax
In most cases it is appropriate to wait for the chest X-ray
to identify a pneumothorax or haemothorax before placing a chest
tube. A haemothorax may also be identified on FAST ultrasound
examination. However there are instances where the patient is
in extremis and it is appropriate to place a chest tube without
waiting for imaging studies. Patients in traumatic arrest with
no cardiac output should have immediate decompression of both
chest hemithoraces to exclude tension pneumothorax. Similarly,
patients in shock or profoundly hypoxic with unilateral chest
signs or evidence of penetrating trauma to a hemithorax should
have a chest drain placed emergently.
Chest tube placement may be diagnostic as well as therapeutic.
After entering the pleural cavity a finger is inserted, and
depending on the position of the tract one may feel the texture
of the lung surface (for contusion), the surface of the diaphragm
(for lacerations) and the heart (for the presence of tamponade).
The nature of the materal draining from the tube is also important.
If it is blood, the chances of requiring a thoracotomy are much
higher if the blood is bright red and arterial rather than the
dark red of venous blood. Drainage of intestinal contents implies
either an oesophageal injury or stomach / bowel injury with
diaphragmatic tear. A persistent air leak implies an underlying
lung laceration, and large leaks may indicate bronchial disruption.
Technique Although often performed in emergent conditions,
attention to technique in placing the chest tube is vital to
avoid complications from the procedure.
Site The chest tube is placed (on the correct side)
in the mid- or anterior- axillary line, behind pectoralis major
(to avoidhaving to dissect through this thick muscle). On expiration,
the diaphragm rises to the 5th rib at the level of the nipple,
and thus chest drains should be placed above this level. Rib
spaces are counted down from the 2nd rib at the sternomanubrial
joint. Practically, the highest rib space that can be easily
felt in the axilla (usually the 4th or 5th) is the most appropriate.
Underwater Seal An underwater seal is used to allow air to escape
through the drain but not to re-enter the thoracic cavity. The
drainage bottle should always be kept below the level of the
patient, otherwise its contents will siphon back into the chest
cavity.Persistent bubbling of air through the water indicates
an air leak from the lung. Chest tubes should NEVER be clamped
for any reason, to avoid the development of a tension pneumothorax.The
air outlet of the underwater seal may be connected to moderate
suction (-20cm water) to assist in lung re-expansion. This is
more important in the presence of an air leak.
Removal Chest drains may be removed when they are no longer
draining any fluid and any air leak has resolved. Removal is
ideally performed with two people - one to remove the tube and
one to occlude the drain site. The tube should be removed either
at the end of expiration or at peak inspiration, to avoid further
air being entrained into the pleural cavity.The area is cleaned
and sterilised. An occlusive dressing is prepared and held ready.
Any stay sutures are removed. With the patient holding his breath
(out or in), the tube removed rapidly and the occlusive dressing
applied.Some surgeons prefer to use a purse-string or U-suture
to close the wound. This may be placed at the time of drain
insertion. While there is no detriment in using a closing suture,
they probably serve little purpose and the purse-string especially
may produce an ugly scar. http://www.trauma.org/archive/thoracic/CHESTdrain.html
Indications * Effusion without a secure clinical diagnosis
(e.g., CHF) or small quantity
* Thoracentesis is a diagnostic procedure done in patients who
have abnormal amounts of fluid accumulation in the pleural space.
* The procedure is usually done at the bedside under local anesthesia.
* The needle is placed through the chest wall into the pleural
space and fluid is then withdrawn into a syringe.
Screening for Thoracentesis
1. History of bleeding disorders or use of anticoagulants
2. Chest x-ray : Make sure that the fluid is not loculated.
This will have a bearing on the Thoracentesis site.
3. Platelet count and PT should be reviewed in patients in whom
you have reason to believe they could be abnormal. It is not
necessary to perform them routinely in other clinical situations.
Selection of Site The posterior approach is superior.
1. The posterior gutter is deep and is the dependent site where
the fluid tends to accumulate in the erect position.
2. The interspaces are wider in the back as compared to the
front.
3. The neurovascular bundle is closer to the inferior margin
of the rib posteriorly. Thus, there is a safer space to enter
the chest.
It is scary to see the needle enter the chest. Hence, the anterior
approach is not preferred.
If we select the axillary approach, it is inconvenient to position
the patient's arm for the duration of the procedure. The arm
will be in the way.
* It is most comfortable to make the patient straddle a chair.
* He should lean forward on a pillow.
* A nurse can stand in front of the patient and hold the patient's
hand.
* We would like to select a site that is dependent and safely
away from important structures. The ideal interspace is the
7th, 8th or 9th space, midway between the posterior axillary
line and midline. This site avoids possible accidental puncture
of the liver, spleen, diaphragm and descending aorta.
* Some experts recommend using the interspace below the upper
limit of dullness.
* Of course, in loculated or small effusions, you will select
the site most likely to yield fluid.
Interpretation
of the ICU Chest Film, Joss D. Fernandez MD, Spencer
B. Gay, MD, Paul M. Dee, MD, Raymond C. Rubner, MD, John M.
Jackson, MEd University of Virginia Health Sciences Center,
Department of Radiology
Hemothorax from Gun Shot Wound
Heliox Therapy
Purpose / Description:
Helium’s density is less than Nitrogen’s, so at
any given gas flow there is less turbulence. This property of
helium can benefit patients with airway obstructions by improving
gas exchange, lowering airway resistance, and reducing work
of breathing.
Indications / Applications of Heliox:
The use of heliox has led to clinical improvement in respiratory
distress and reduced work of breathing in a variety of obstructive
lesions including:
1. Upper Airway Obstruction:
a. Viral & post-extubation croup
b. Anaphylaxis
c. Vocal cord paralysis
d. Upper airway masses, including tumors
2. Lower Airway Obstruction
a. Asthma
b. COPD
c. Brochiolitis
d. Bronchopulmonary dysplasia
Heliox Therapy in Acute Severe Asthma, Jonathan E. Kass,
MD, FCCP; and Richard J. Castriotta, MD, FCCP
Barachl in 1935 was the first to use helium to improve air flow
in patients with airways obstruction, but it was soon cast aside
for other treatment modalities. Since then, it has been relegated
mainly to use in upper airway obstruction or to diagnostic studies.
Safety and efficacy have been demonstrated for both spontaneously
breathing patients and for intubated patients receiving mechanical
ventilation, but its therapeutic potential has not been fully
explored. Helium has no bronchodilating or anti-inflammatory
properties and in fact is quite inert. Since airway resistance
in turbulent flow is directly related to the density of the
gas, helium, with its lower density than nitrogen or oxygen,
results in lower airway resistance. Helium further lowers airway
resistance by reducing the Reynolds number, such that some areas
of turbulent flow are converted to laminar flow. The reduction
in airway resistance results in a decreased work of breathing.
Although the mortality from asthma is rising, there has been
a paucity of new treatments for acute severe asthma. Previous
reports have shown an almost universal response to heliox in
acute severe asthma. We wish to report our experience with heliox
and our attempt to better define its utility by discerning patterns
of response.
Heliox During Mechanical Ventilation, Shekhar T Venkataraman
MD
The indications for heliox during mechanical ventilation are
lower-airway obstruction, especially with hypercarbia; need
to enhance aerosol delivery to lung periphery; and need to facilitate
weaning from mechanical ventilation. Certain ventilators perform
relatively well with heliox and are not substantially affected
by it. It is preferable to connect the heliox to the air inlet
of the ventilator, because this results in more consistent delivery
of oxygen and tidal volume. When administering heliox, pay close
attention and directly monitor the actual tidal volume and fraction
of inspired oxygen.
Respiratory Emergencies in Children, Alexandre T Rotta
MD and Budi Wiryawan MD The administration of a mixture of helium and oxygen (heliox)
can be of benefit in the treatment of selected patients with
severe forms of LTB. Helium is a very light, odorless, tasteless,
noncombustible, and physiologically inert gas. It is has a very
low gas density (0.1785 g/L) in comparison to room air (1.20
g/L). Therefore, a mixture of helium and oxygen can create a
respirable gas with a density lower that of an oxygen/nitrogen
mixture or oxygen alone (1.43 g/L). The low density of heliox
reduces the gas turbulence in the airways (and around the obstruction)
and the pressure gradient needed to generate respiratory flow,
thus decreasing the work of breathing and benefiting the patient
who is suffering an airway obstruction. Effective mixtures of
helium and oxygen contain between 80:20 and 60:40 parts of each
gas, respectively. Therefore, patients with a high oxygen requirement
(greater than 40%) are unlikely to benefit from this therapy.
Heliox should only be administered from a pre-mixed heliox cylinder
with 80% helium and 20% oxygen, so as to prevent the possibility
of asphyxia by accidentally delivering 100% helium, as would
be the case if the oxygen cylinder were empty. Higher oxygen
concentration can be obtained by blending in oxygen from an
oxygen cylinder with the heliox
G. AIRWAY MANAGEMENT
CPR (Adult)
* Airway
* Breathing
* Circulation
AIRWAY
"A" is for AIRWAY. If the victim
is unconscious and is unresponsive, you need to make sure that
his airway is clear of any obstructions. The breaths may be
faint and shallow - look, listen and feel for any signs of breathing.
If you determine that the victim is not breathing, then something
may be blocking his air passage. The tongue is the most common
airway obstruction in an unconscious person.
With the victim lying flat on his back, place your hand on
his forehead and your other hand under the tip of the chin (Figure
1). Gently tilt the victim's head backward. In this position
the weight of the tongue will force it to shift away from the
back of the throat, opening the airway (Figure 2).
If the person is still not breathing on his own after the airway
has been cleared, you will have to assist him breathing
BREATHING
"B" is for BREATHING. With the victim's
airway clear of any obstructions, gently support his chin so
as to keep it lifted up and the head tilted back. Pinch his
nose with your fingertips to prevent air from escaping once
you begin to ventilate and place your mouth over the victim's,
creating a tight seal (Figure 1).
As you assist the person in breathing, keep an eye on his chest.
Try not to over-inflate the victim's lungs as this may force
air into the stomach, causing him to vomit. If this happens,
turn the person's head to the side and sweep any obstructions
out of the mouth before proceeding.
Give two full breaths. Between each breath allow the victim's
lungs to relax - place your ear near his mouth and listen for
air to escape and watch the chest fall as the victim exhales
(Figure 2).
If the victim remains unresponsive (no breathing, coughing
or moving), check his circulation
CIRCULATION
"C" is for CIRCULATION. In order
to determine if the victim's heart is beating, place two fingertips
on his carotid artery, located in the depression between the
windpipe and the neck muscles (Figure 1), and apply slight pressure
for several seconds.
If there is no pulse then the victim's heart is not beating,
and you will have to perform chest compressions
When performing chest compressions, proper hand placement is
very important. To locate the correct hand position place two
fingers at the sternum (the spot where the lower ribs meet)
then put the heel of your other hand next to your fingers (Figure
1).
Place one hand on top of the other and interlace the fingers
(Figure 2). Lock your elbows and using your body's weight, compress
the victim’s chest. The depth of compressions should be
approximately 1½ to 2 inches - remember: 2 hands, 2 inches
(Figure 3). If you feel or hear slight cracking sound, you may
be pressing too hard. Do not become alarmed and do not stop
your rescue efforts! Damaged cartilage or cracked ribs are far
less serious than a lost life. Simply apply less pressure as
you continue compressions.
Count aloud as you compress 30 times at the rate of about 3
compressions for every 2 seconds. Finish the cycle by giving
the victim 2 breaths. This process should be performed four
times - 30 compressions and 2 breaths - after which remember
to check the victim's carotid artery for pulse and any signs
of consciousness.
If there is no pulse, continue performing 30 compressions/2
breaths, checking for pulse after every 4 cycles until help
arrives.
If you feel a pulse (i.e. the victim's heart is beating) but
the victim is still not breathing, rescue breaths should be
administered, one rescue breath every five seconds (remember
to pinch the nose to prevent air from escaping). After the first
rescue breath, count five seconds and if the victim does not
take a breath on his own, give another rescue breath.



 Droplet Precautions are intended to prevent transmission of
pathogens spread through close respiratory or mucous membrane
contact with respiratory secretions.. Because these pathogens
do not remain infectious over long distances in a healthcare
facility, special air handling and ventilation are not required
to prevent droplet transmission. Droplet Precautions are indicated
are for conditions such as. pertussis, influenza virus, adenovirus,
rhinovirus, N. meningitides, and group A streptococcus.Healthcare
personnel wear a mask (a respirator is not necessary) for close
contact with infectious patient; the mask is generally donned
upon room entry. Patients on Droplet Precautions who must be
transported outside of the room should wear a mask if tolerated
and follow Respiratory Hygiene/Cough Etiquette. Use Droplet
Precautions for patients known or suspected to be infected with
pathogens transmitted by respiratory droplets (i.e., large-particle
droplets >5µ in size) that are generated by a patient
who is coughing, sneezing or talking.
Droplet Precautions are intended to prevent transmission of
pathogens spread through close respiratory or mucous membrane
contact with respiratory secretions.. Because these pathogens
do not remain infectious over long distances in a healthcare
facility, special air handling and ventilation are not required
to prevent droplet transmission. Droplet Precautions are indicated
are for conditions such as. pertussis, influenza virus, adenovirus,
rhinovirus, N. meningitides, and group A streptococcus.Healthcare
personnel wear a mask (a respirator is not necessary) for close
contact with infectious patient; the mask is generally donned
upon room entry. Patients on Droplet Precautions who must be
transported outside of the room should wear a mask if tolerated
and follow Respiratory Hygiene/Cough Etiquette. Use Droplet
Precautions for patients known or suspected to be infected with
pathogens transmitted by respiratory droplets (i.e., large-particle
droplets >5µ in size) that are generated by a patient
who is coughing, sneezing or talking.
 Airborne Precautions prevent transmission of infectious agents
that remain infectious over long distances when suspended in
the air (e.g., rubeola virus [measles], varicella virus [chickenpox],
Mycobacterium. tuberculosis, and possibly SARS-CoV). The preferred
placement for patients who require Airborne Precautions is in
an airborne infection isolation room (AIIR). An AIIR is a single-patient
room that is equipped with special air handling and ventilation
capacity that meet the American Institute of Architects/Facility
Guidelines Institute (AIA/FGI) standards for AIIRs (i.e., monitored
negative pressure relative to the surrounding area, 12 air exchanges
per hour for new construction and renovation and 6 air exchanges
per hour for existing facilities, air exhausted directly to
the outside or recirculated through HEPA filtration before return).In
settings where Airborne Precautions cannot be implemented due
to limited engineering resources (e.g., physician offices),
masking the patient, placing the patient in a private room (e.g.,
office examination room) with the door closed, and providing
N95 or higher level respirators or masks if respirators are
not available for healthcare personnel will reduce the likelihood
of airborne transmission until the patient is either transferred
to a facility with an AIIR or returned to the home environment,
as deemed medically appropriate. Whenever possible, non-immune
HCWs should not care for patients with vaccine-preventable airborne
diseases (e.g., measles, chickenpox, and smallpox).(
Airborne Precautions prevent transmission of infectious agents
that remain infectious over long distances when suspended in
the air (e.g., rubeola virus [measles], varicella virus [chickenpox],
Mycobacterium. tuberculosis, and possibly SARS-CoV). The preferred
placement for patients who require Airborne Precautions is in
an airborne infection isolation room (AIIR). An AIIR is a single-patient
room that is equipped with special air handling and ventilation
capacity that meet the American Institute of Architects/Facility
Guidelines Institute (AIA/FGI) standards for AIIRs (i.e., monitored
negative pressure relative to the surrounding area, 12 air exchanges
per hour for new construction and renovation and 6 air exchanges
per hour for existing facilities, air exhausted directly to
the outside or recirculated through HEPA filtration before return).In
settings where Airborne Precautions cannot be implemented due
to limited engineering resources (e.g., physician offices),
masking the patient, placing the patient in a private room (e.g.,
office examination room) with the door closed, and providing
N95 or higher level respirators or masks if respirators are
not available for healthcare personnel will reduce the likelihood
of airborne transmission until the patient is either transferred
to a facility with an AIIR or returned to the home environment,
as deemed medically appropriate. Whenever possible, non-immune
HCWs should not care for patients with vaccine-preventable airborne
diseases (e.g., measles, chickenpox, and smallpox).(








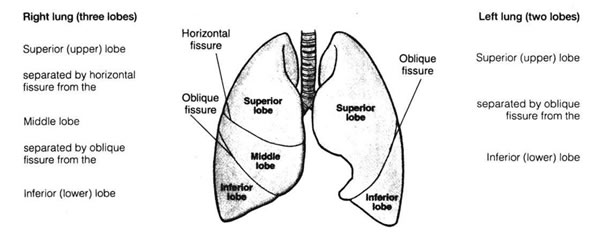


















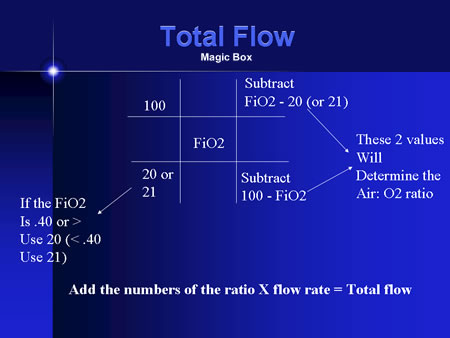
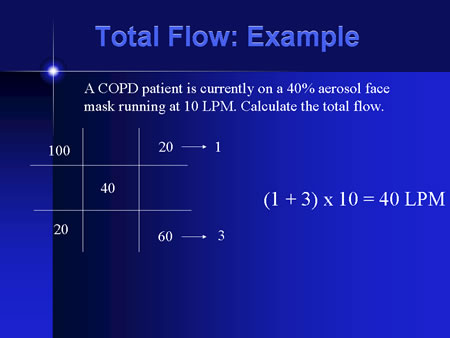
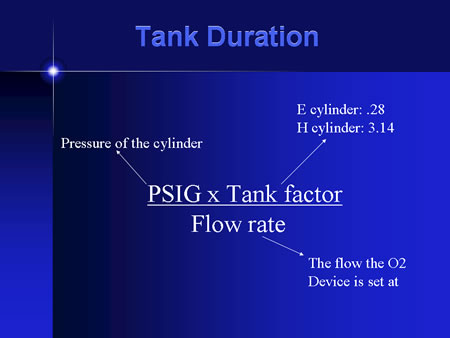
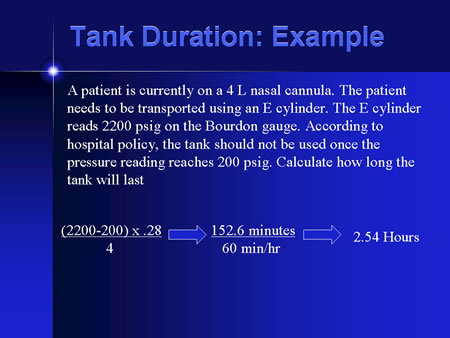
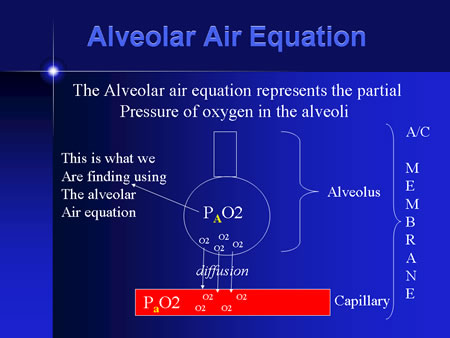
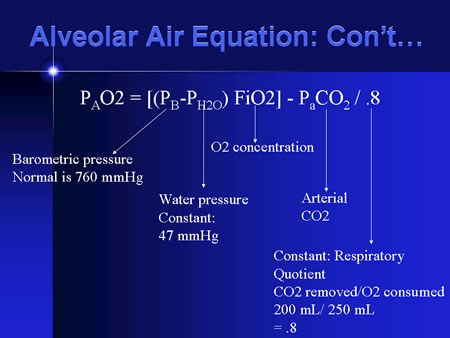
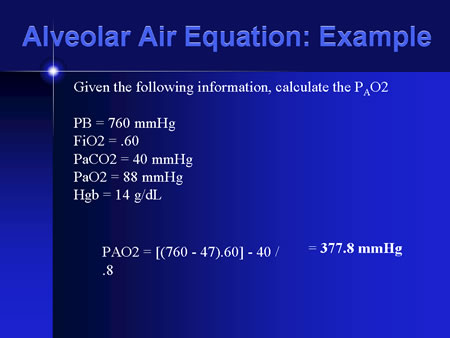
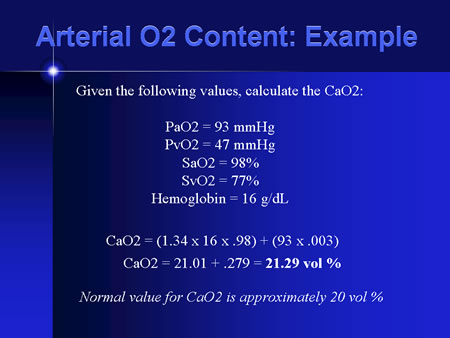
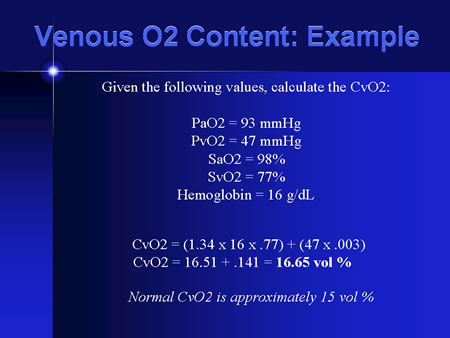
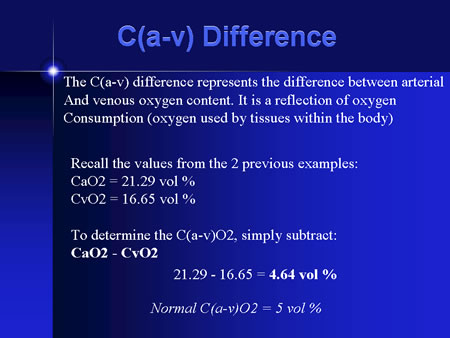
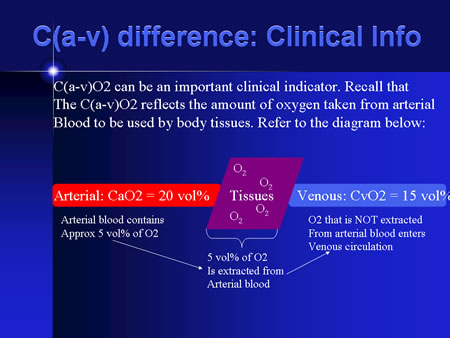



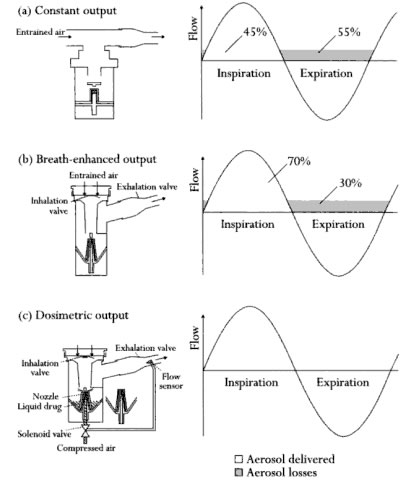




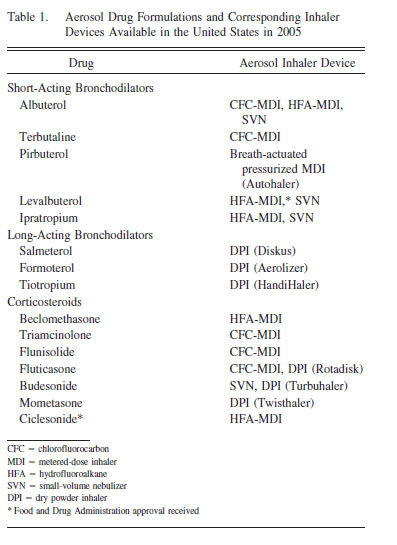






























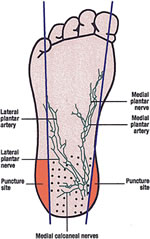





 Capnography Learning Website
Capnography Learning Website



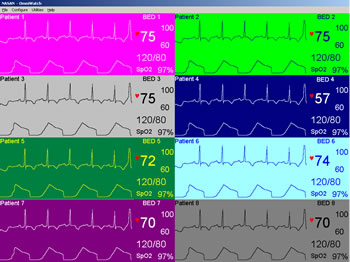



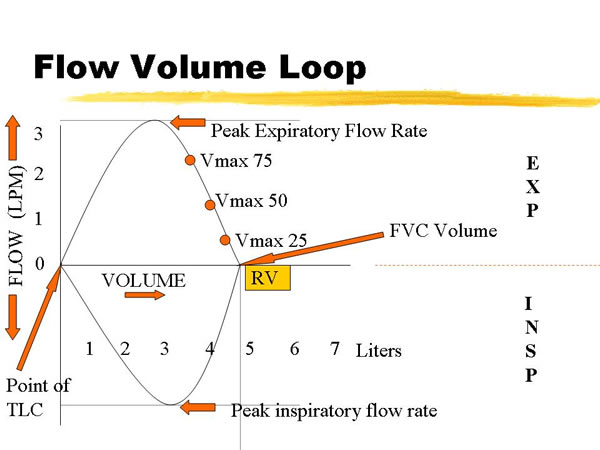
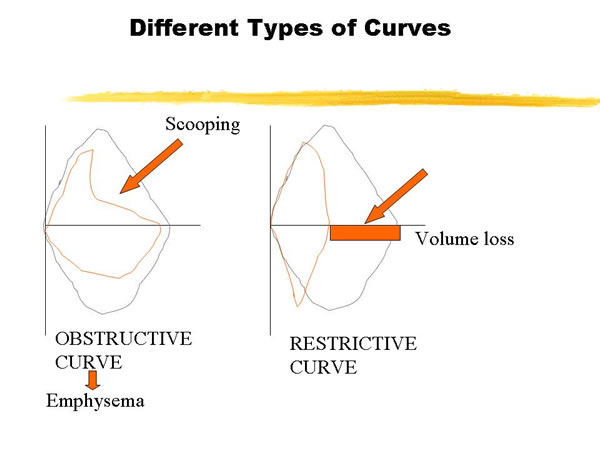
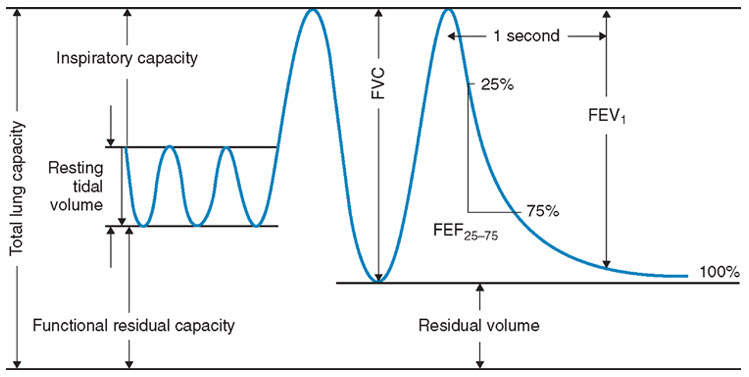
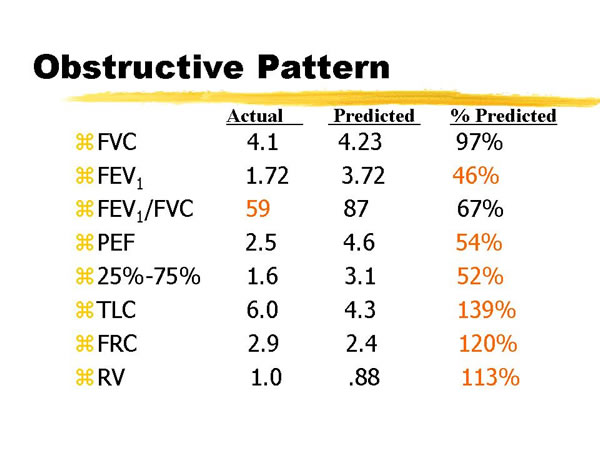
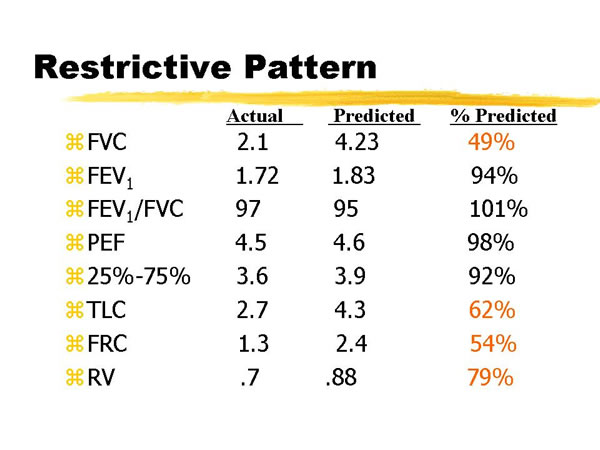




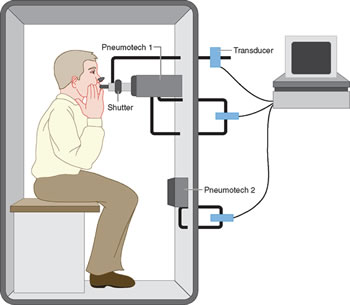



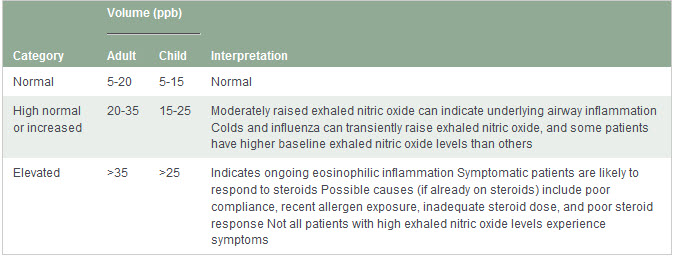
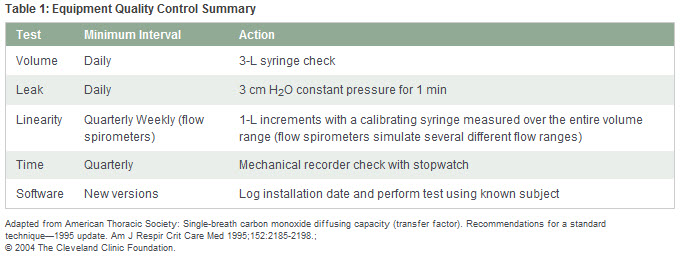
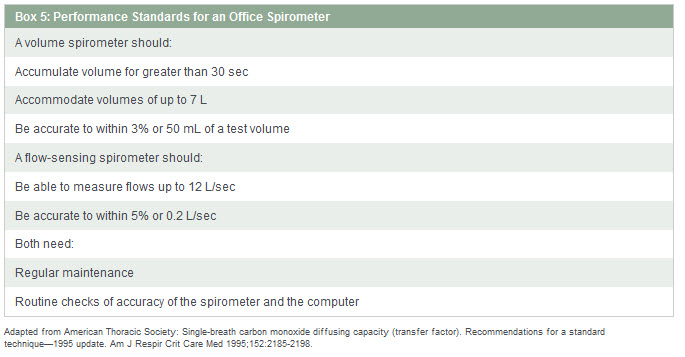
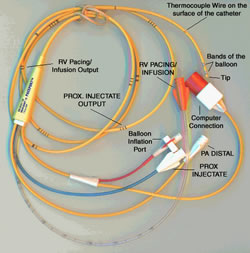
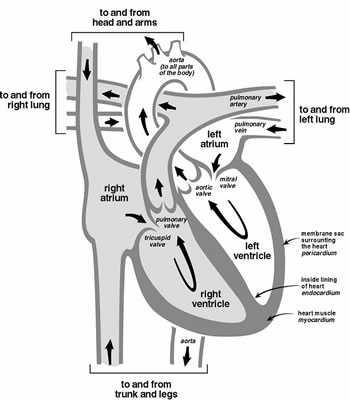



 Basic Chest
X-Ray Interpretation,
Basic Chest
X-Ray Interpretation, Interpretation
of the ICU Chest Film
Interpretation
of the ICU Chest Film

{kind=link}